Download to read offline




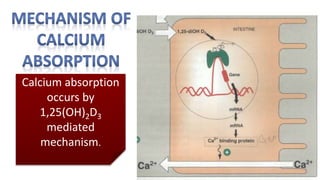

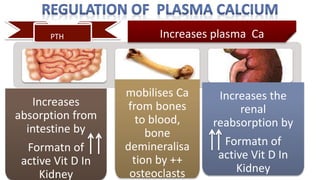
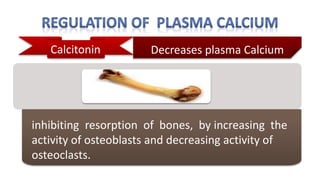
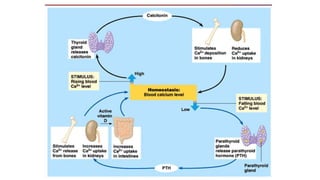

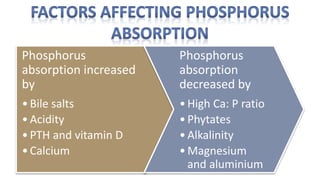
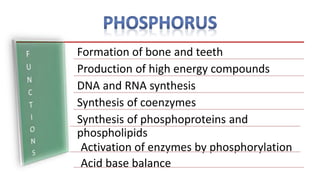
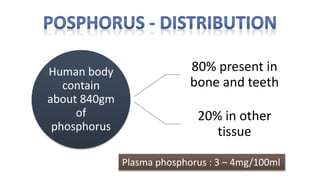
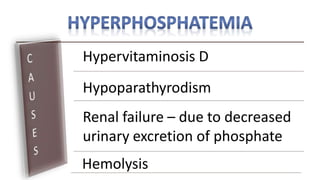
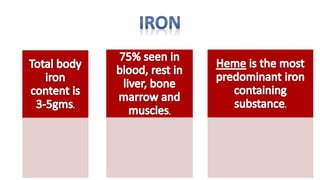
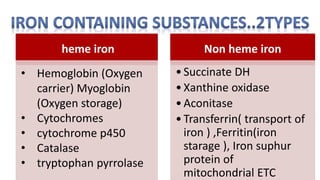

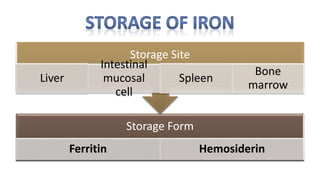
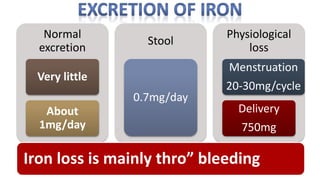


A 32-year-old vegetarian school teacher presented with symptoms of fatigue, breathlessness, and pallor, revealing severe anemia with a hemoglobin level of 7.5 g/dl. The document details the importance of minerals like calcium and phosphorus in the body, their sources, absorption mechanisms, and effects of deficiency or excess, highlighting the role of specific hormones in regulating these minerals. It also discusses the functions and absorption of iron, distinguishing between heme and non-heme iron, and the consequences of iron deficiency and overload.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

