
![Department of Defense HIV/AIDS Prevention Program
Military International HIV Training Program (MIHTP)
ECHO Rounds (Module 10)
.
Tuesday, April 27, 2021
.
07:00-08:30 (San Diego, CA, USA, UTC -8)
15:00-16:30 Republic of the Congo, Brazzaville [WAT; UTC+0100]
16:00-17:30 South Africa, Johannesburg [SAST; UTC+0200]
17:00-18:30 Kenya, Nairobi [EAT; UTC+0300]
2:00pm-3:30 pm (Coordinated Universal Time, UTC) 3](https://image.slidesharecdn.com/mihtp-echo27aprenglishfinal2-210502190920/75/Military-International-HIV-Training-Program-MIHTP-ECHO-Rounds-April-27-2021-3-2048.jpg)

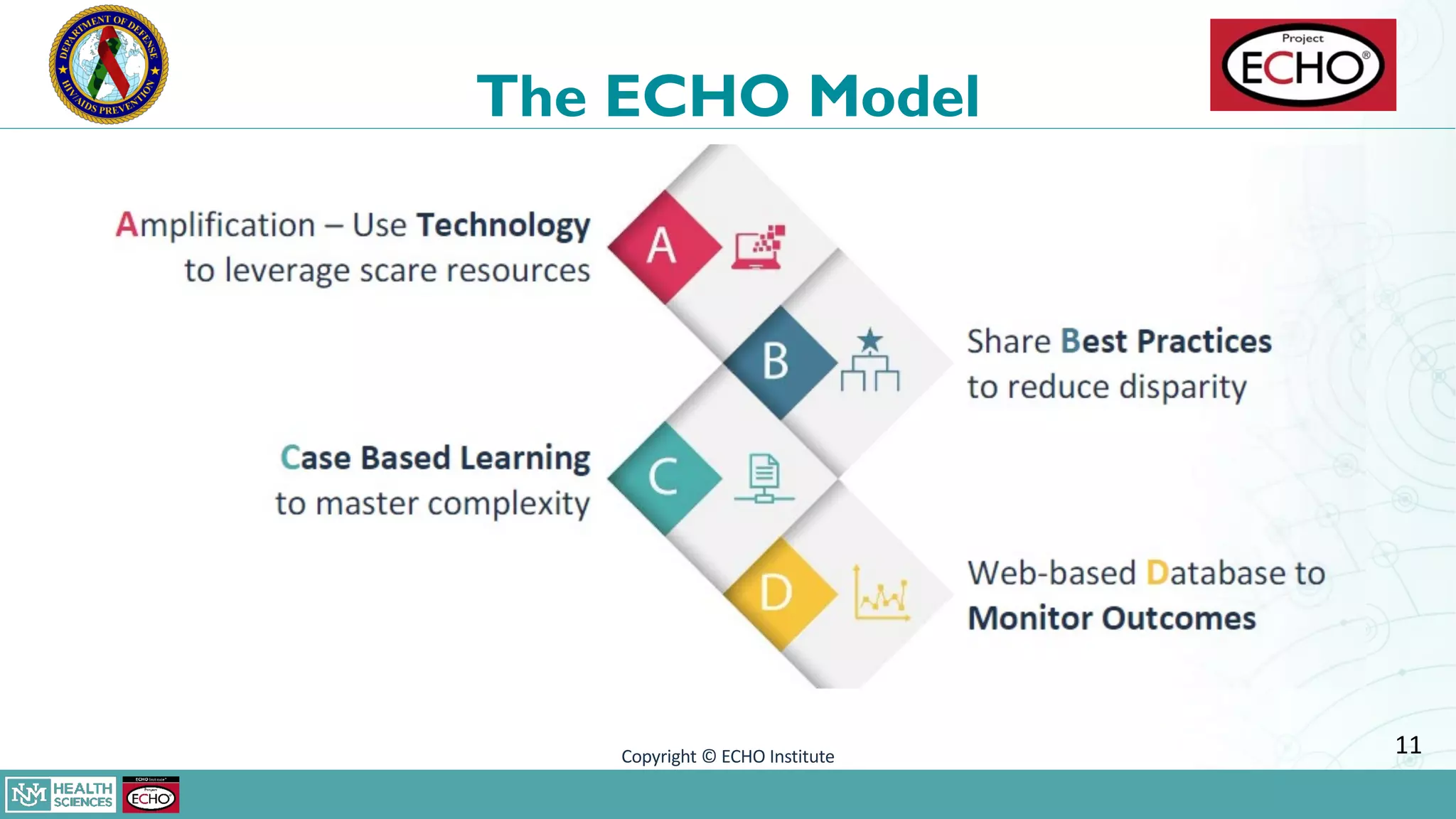
![ECHO Introduction
Project ECHO® [Extension for Community Healthcare Outcomes] is a model of
distance clinical mentorship developed at the University of New Mexico to
improve access to care for complex health problems for underserved
populations.
Elements of the model include:
• Hub-and-spoke networks
• Communities of Practice
• Didactics and case-based learning
• Chronic disease management
10](https://image.slidesharecdn.com/mihtp-echo27aprenglishfinal2-210502190920/75/Military-International-HIV-Training-Program-MIHTP-ECHO-Rounds-April-27-2021-10-2048.jpg)















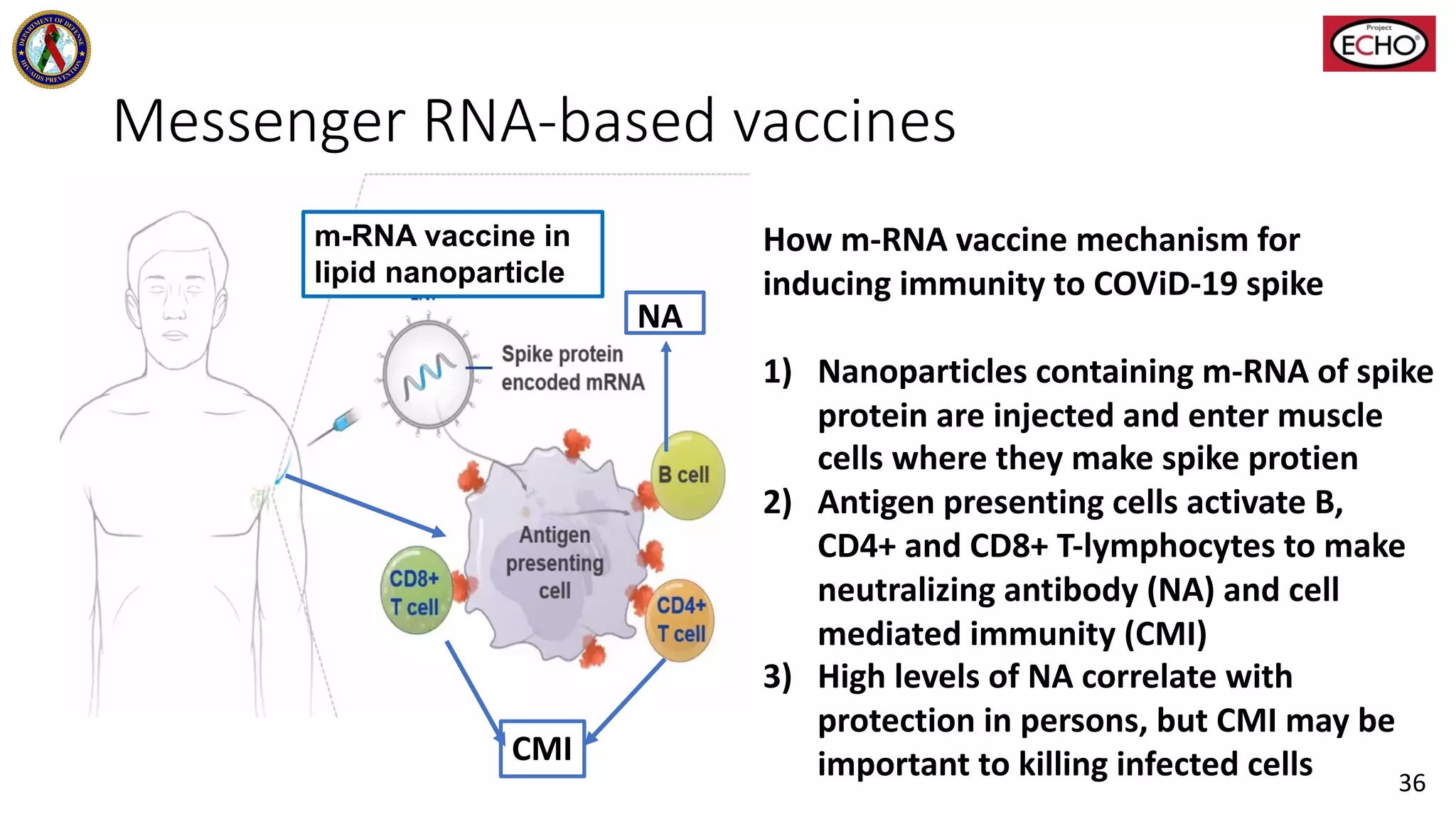

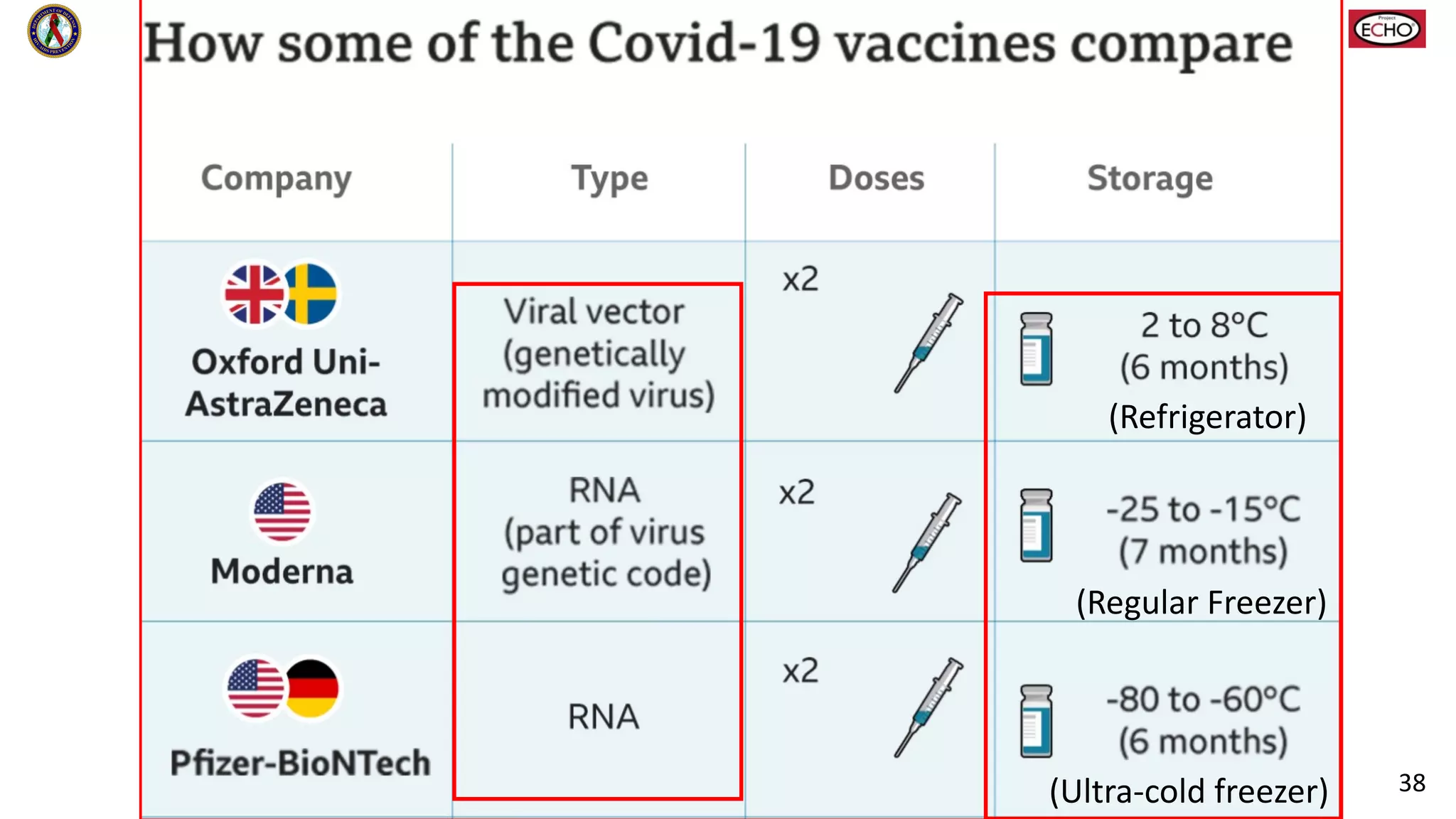

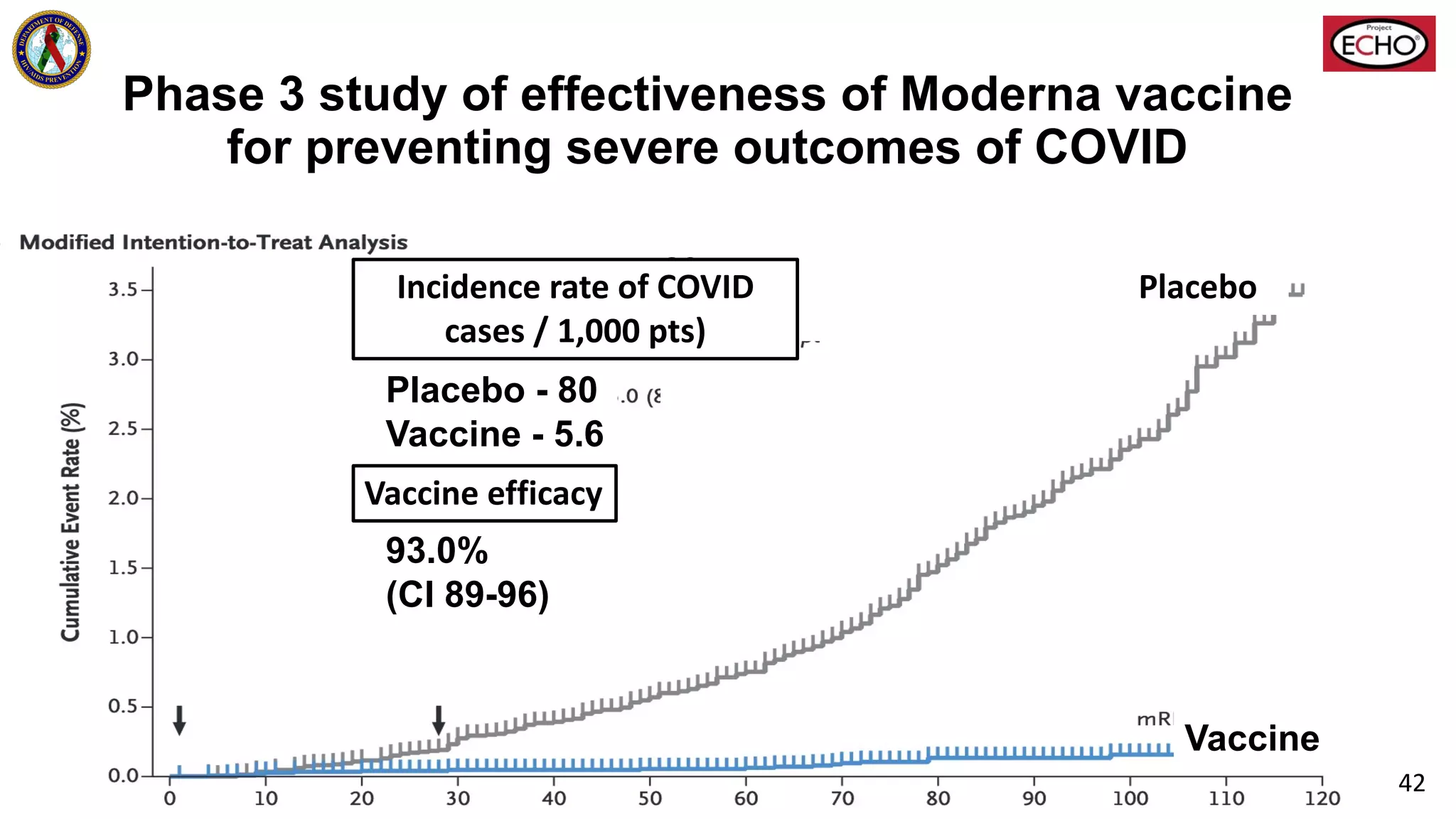






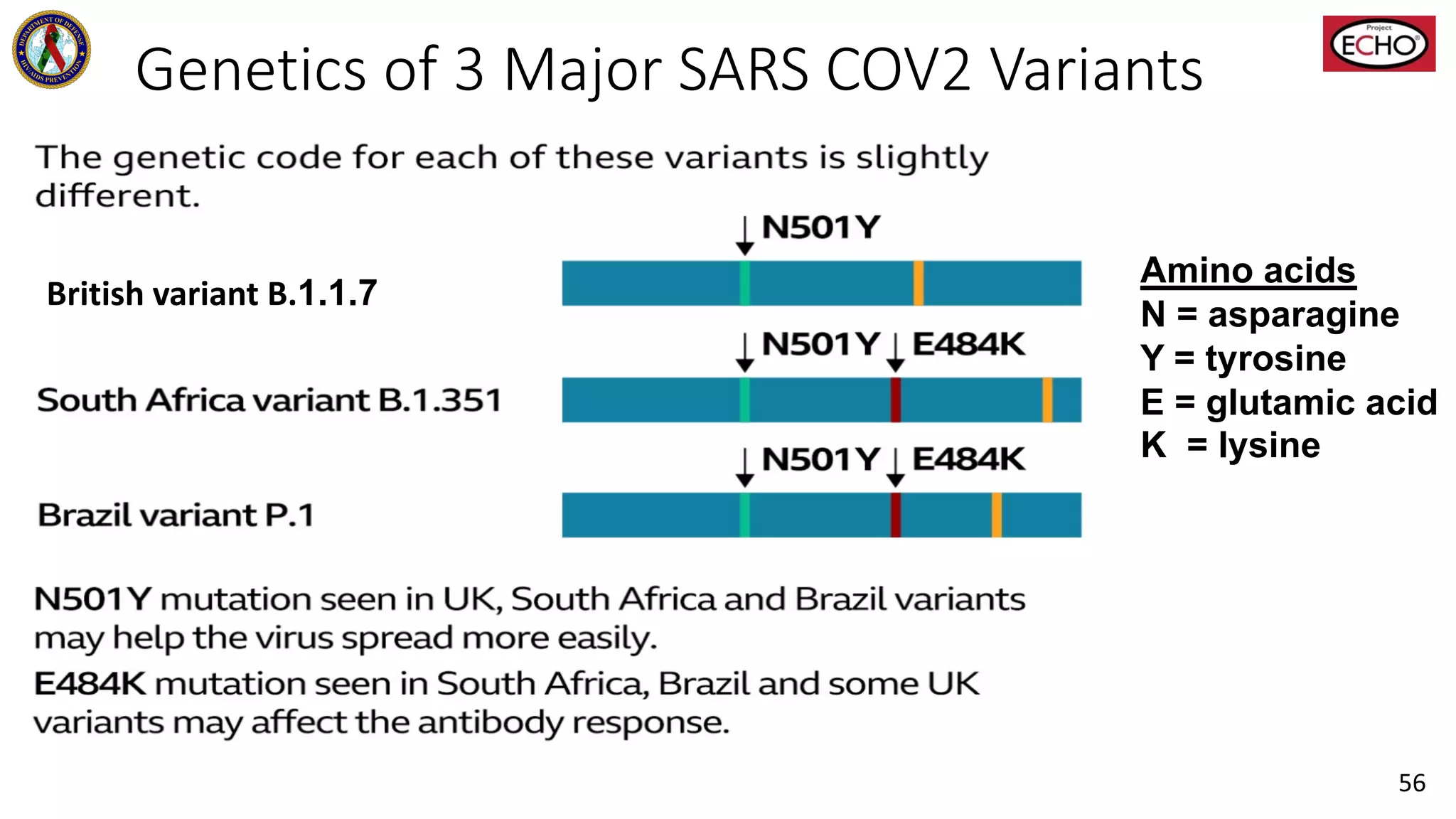






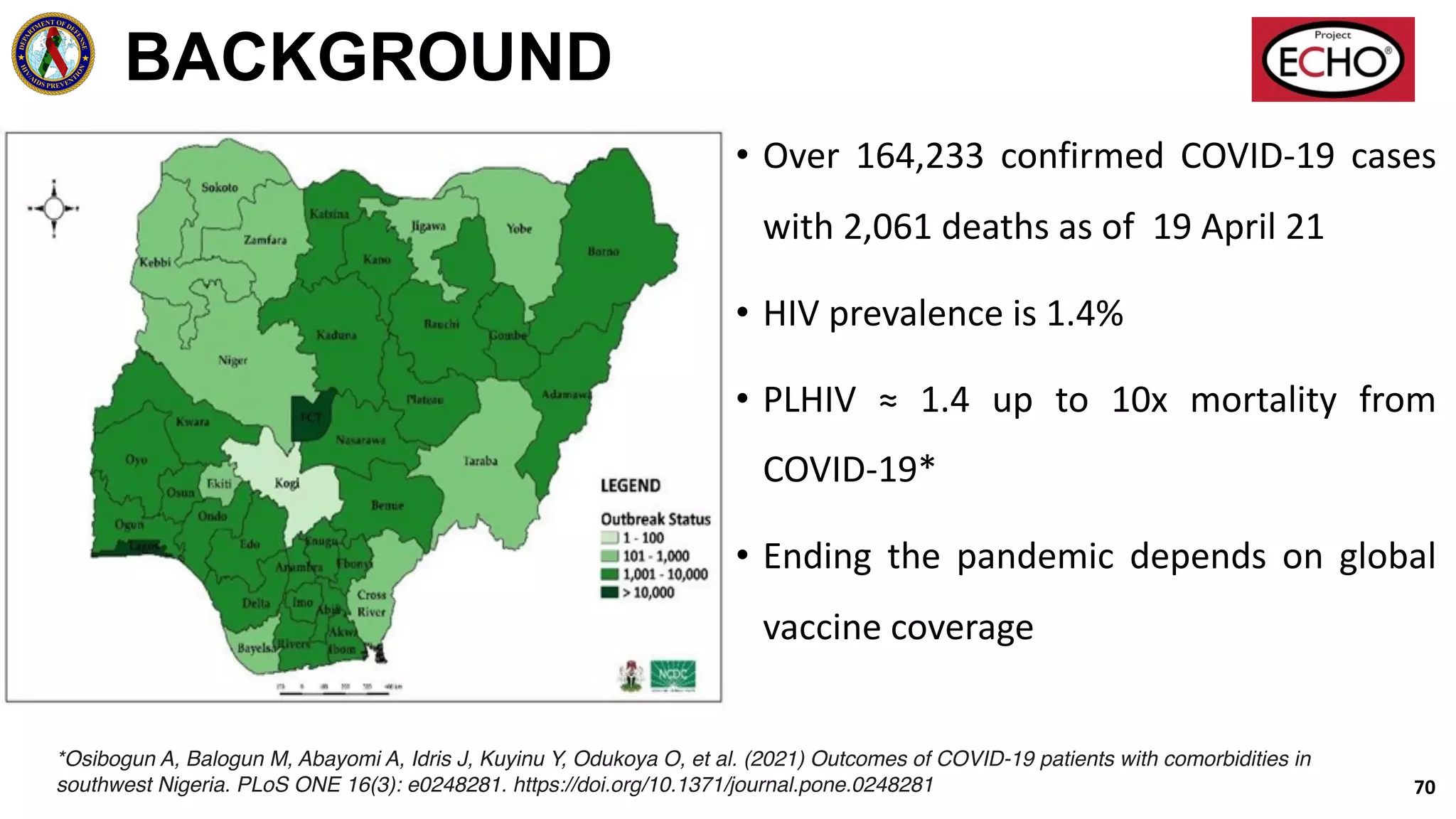
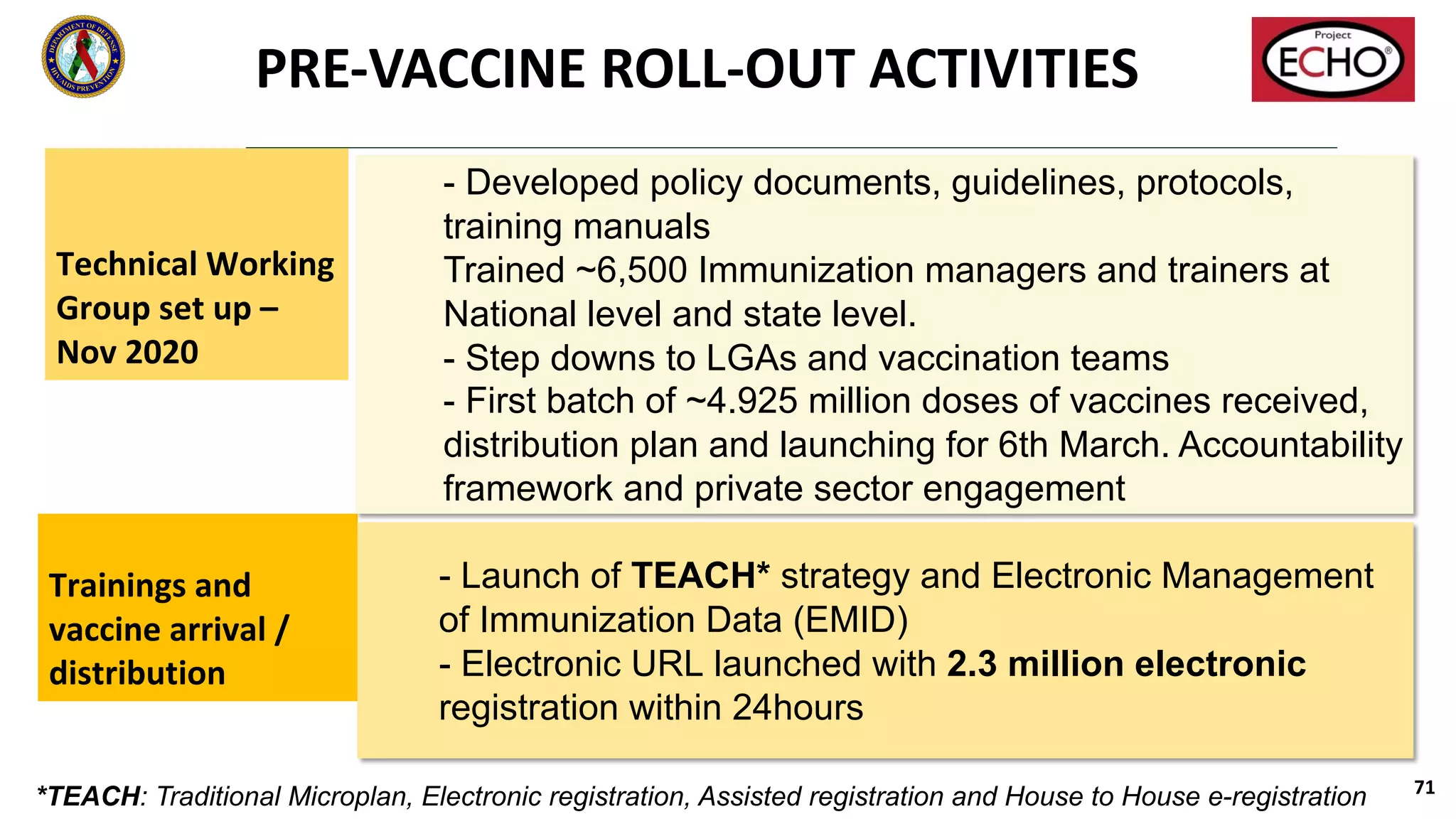
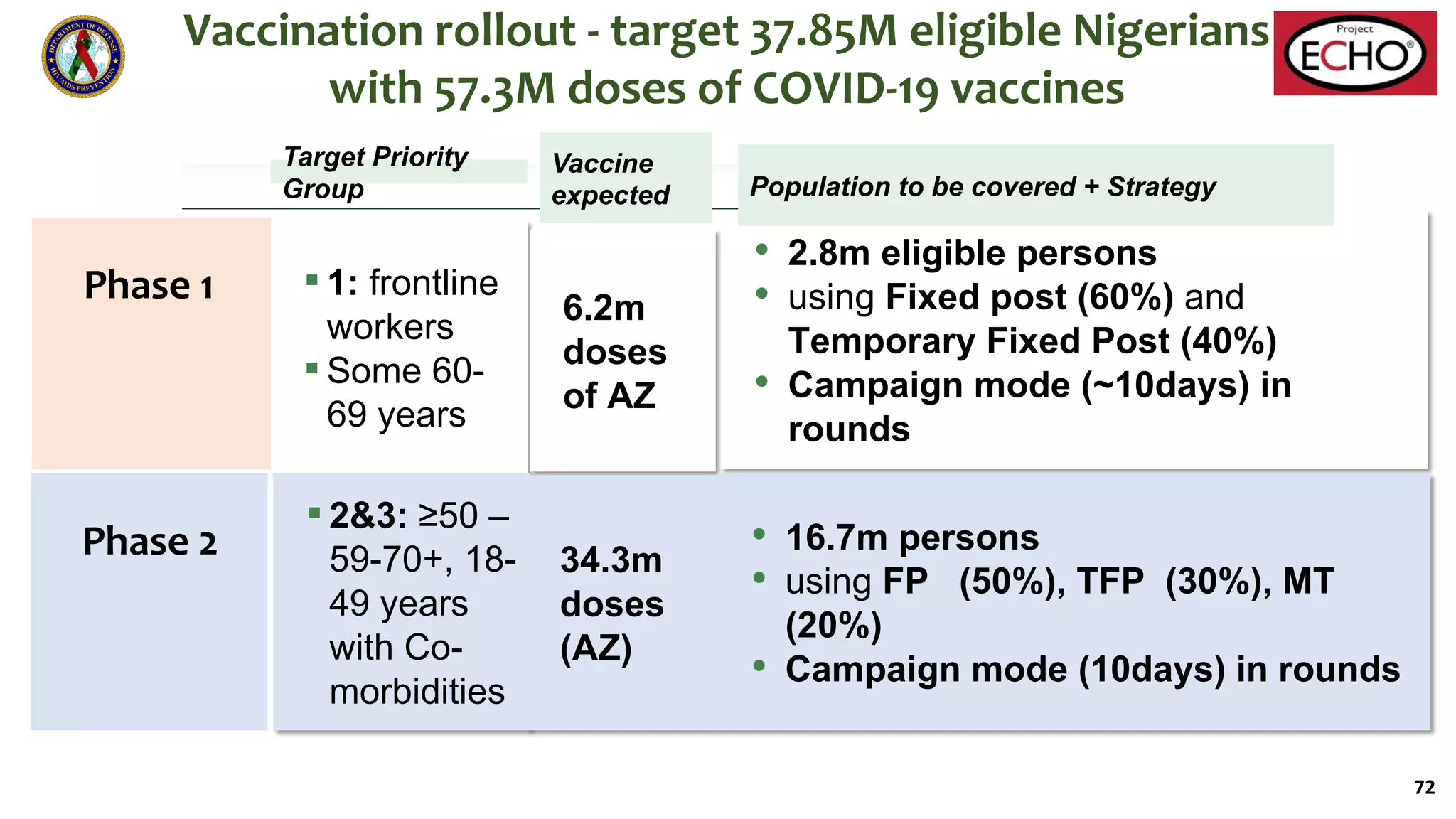

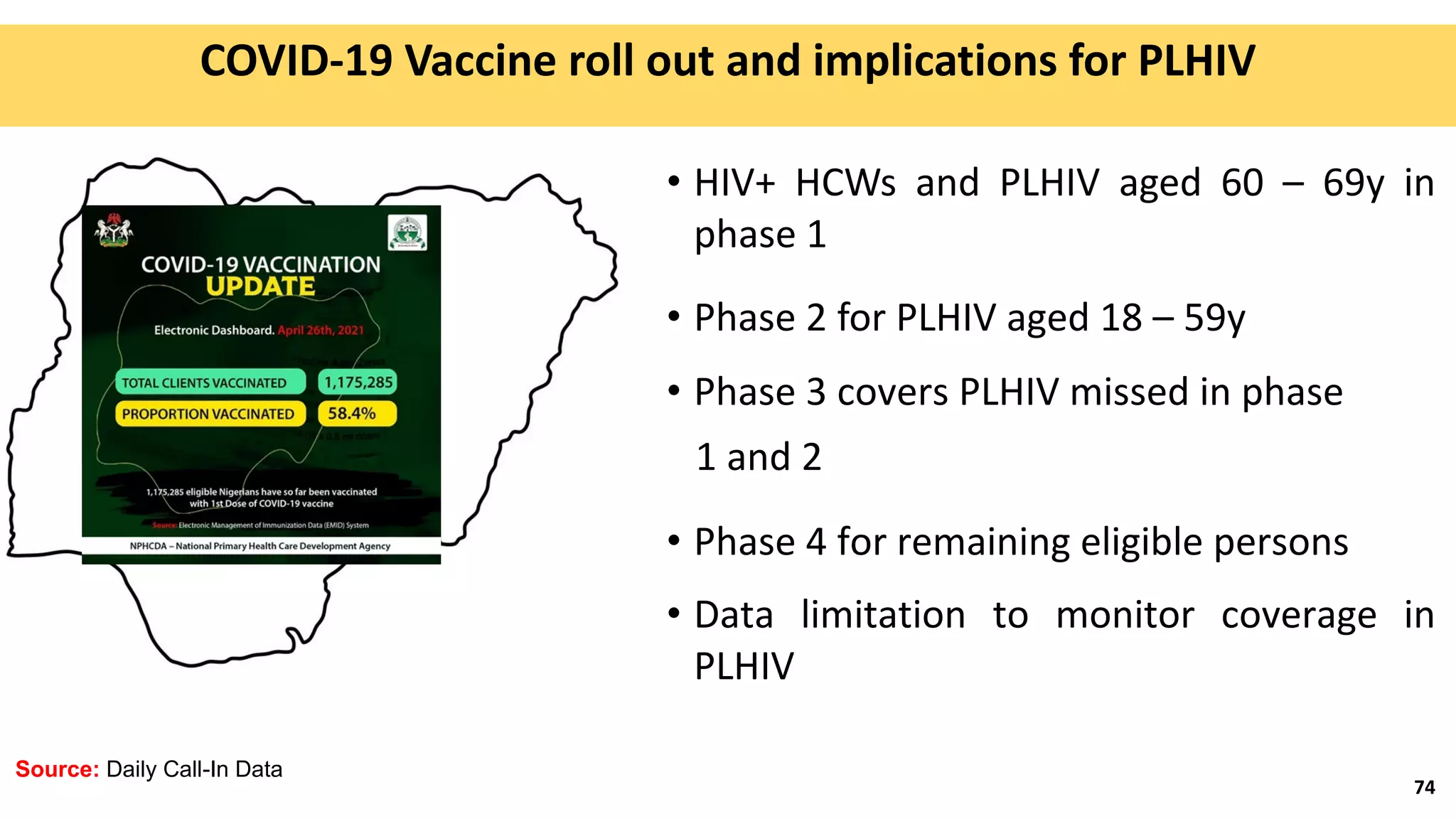



This document provides information about a MIHTP-ECHO training session on COVID-19 vaccines. It includes the agenda, presenters, and an overview of MIHTP and the ECHO model. The presentation by Dr. Allen McCutchan will discuss COVID epidemiology, vaccine mechanisms of action, effectiveness, safety, and duration of protection. It will also cover implications for people living with HIV and emerging variants. A presentation by Captain UO Adekanye will provide an update on Nigeria's COVID vaccine rollout and implications for people living with HIV. The session aims to inform participants and facilitate discussion on these topics.



































































