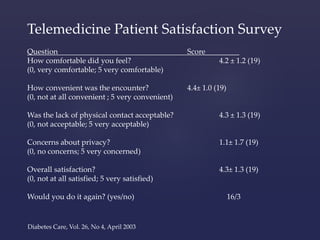
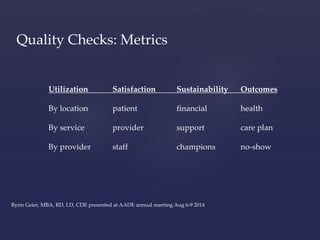
The document discusses the benefits and components of a diabetes telehealth program, emphasizing its effectiveness in improving diabetes management and patient education. It outlines the selection process for telehealth programs, budget considerations, and the importance of provider and patient engagement. Additional insights include patient satisfaction metrics and evidence of cost reduction and improved access to care through the telehealth model.