Downloaded 20 times


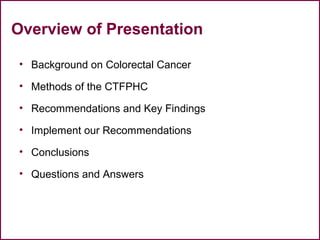
![A Model for Evidence-
Informed Decision Making
National Collaborating Centre for Methods and Tools. (revised 2012). A
Model for Evidence-Informed Decision-Making in Public Health (Fact
Sheet). [http://www.nccmt.ca/pubs/FactSheet_EIDM_EN_WEB.pdf]](https://image.slidesharecdn.com/healthevidencewebinar-mariadonna-may162016-160518194925/85/Colorectal-screening-evidence-colonoscopy-screening-guidelines-12-320.jpg)
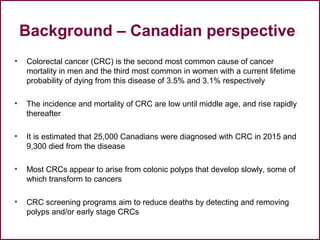
![Stages in the process of Evidence-
Informed Public Health
National Collaborating Centre for Methods and Tools. Evidence-Informed
Public Health. [http://www.nccmt.ca/eiph/index-eng.html]](https://image.slidesharecdn.com/healthevidencewebinar-mariadonna-may162016-160518194925/85/Colorectal-screening-evidence-colonoscopy-screening-guidelines-13-320.jpg)
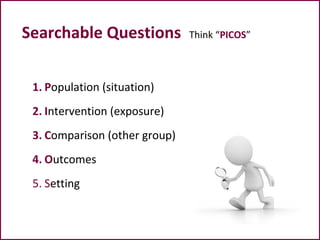




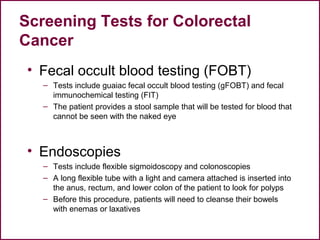
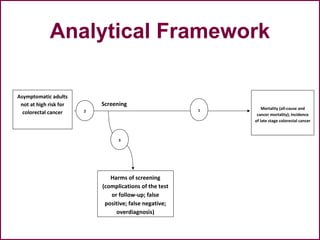
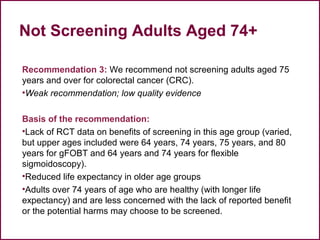
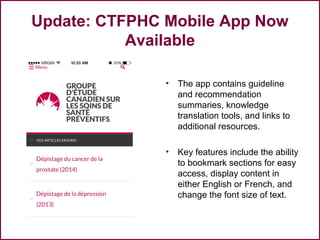
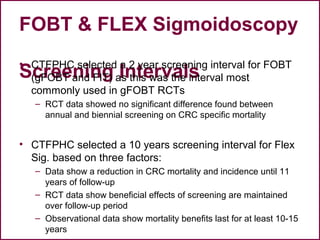
![P Asymptomatic adults 18 years and older who are not at high risk of
colorectal cancer
I
Screening with colonoscopy, CT colonography, gFOBT, iFOBT, FS, BE, DRE,
fecal DNA, serum DNA, other identified tests currently being used for
screening in Canada
C
• No screening
• Head to head – two tests compared with each other
O
Mortality (all-cause and colorectal cancer-specific)
Incidence of late stage colorectal cancer (stage III or IV; or Duke’s C or D)
Sensitivity, specificity, negative and positive predictive value for detection of
any stage colorectal cancer for those tests with evidence for screening
effectiveness
Harms: complications (bleeding [not requiring hospitalization and requiring
hospitalization], perforation, death) of the test or follow-up test, false
positive, false negative, overdiagnosis
S Primary care, including referrals for tests by primary care practitioners](https://image.slidesharecdn.com/healthevidencewebinar-mariadonna-may162016-160518194925/85/Colorectal-screening-evidence-colonoscopy-screening-guidelines-29-320.jpg)

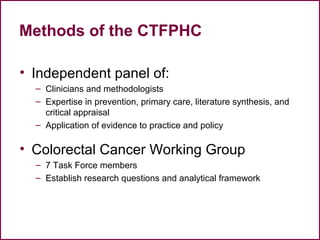
![A Model for Evidence-
Informed Decision Making
National Collaborating Centre for Methods and Tools. (revised 2012). A
Model for Evidence-Informed Decision-Making in Public Health (Fact
Sheet). [http://www.nccmt.ca/pubs/FactSheet_EIDM_EN_WEB.pdf]](https://image.slidesharecdn.com/healthevidencewebinar-mariadonna-may162016-160518194925/85/Colorectal-screening-evidence-colonoscopy-screening-guidelines-62-320.jpg)

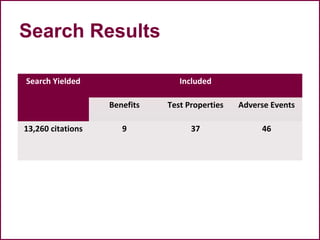
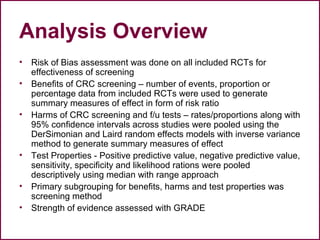
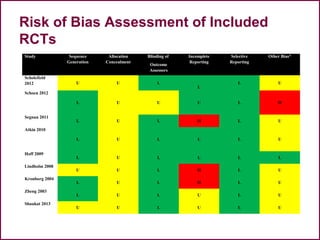
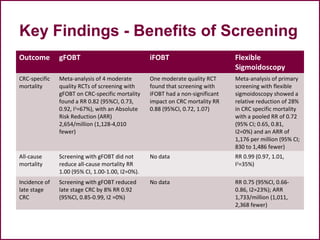
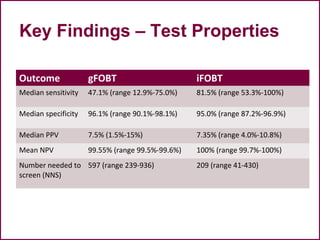
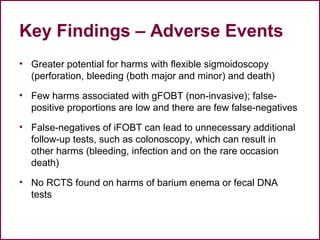
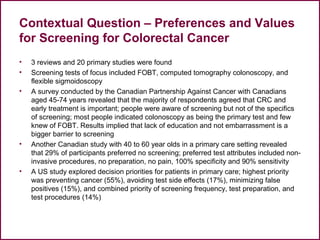
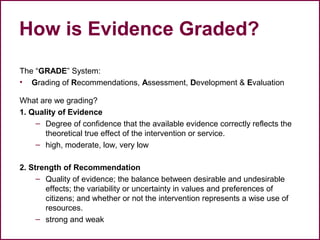
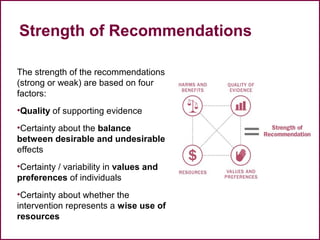
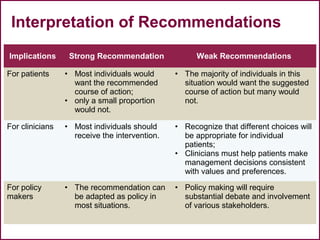
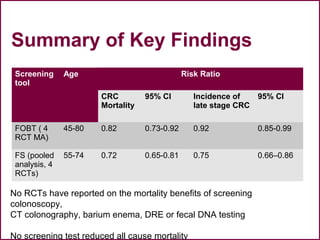
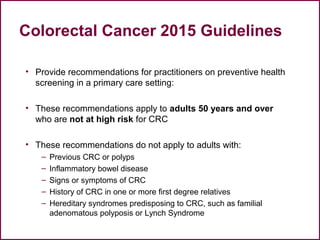
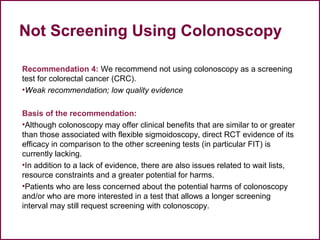
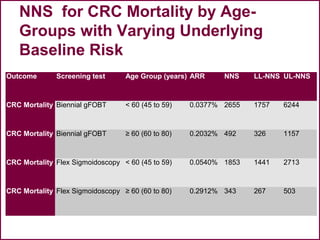
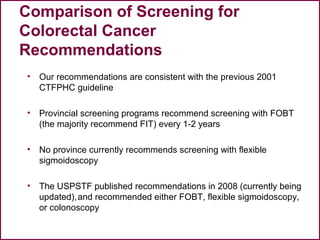
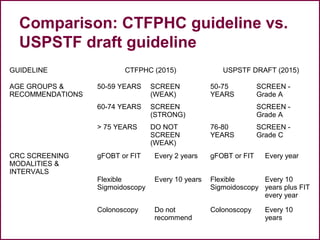
The document discusses colorectal cancer screening guidelines intended for professional development, focusing on recommendations for screening asymptomatic adults aged 50 and older. It outlines evidence supporting screening methods, the effectiveness and risks of various tests, and emphasizes the importance of informed decision-making by practitioners and patients. Additionally, it highlights the role of systematic reviews in guiding these recommendations while providing resources for further information.









































































































