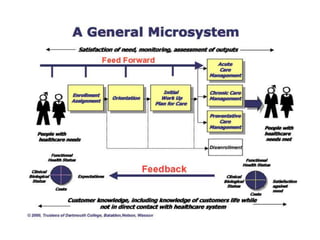
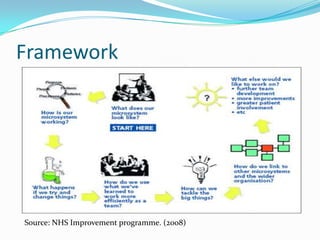
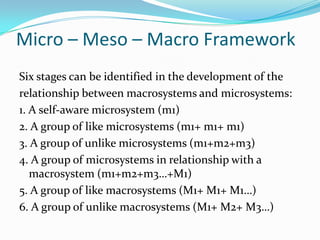
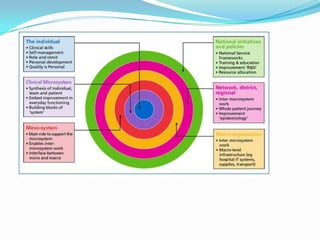
This document discusses clinical microsystems, which are small groups of healthcare professionals and staff who work together to provide care for a defined patient population. A clinical microsystem has shared goals, processes, an information environment, and is responsible for performance outcomes. The document outlines the key components of a microsystem, including its purpose, patients, staff, processes, and patterns. It also discusses how microsystems relate to larger macrosystems in a healthcare organization and the benefits of using a microsystem approach to improve care quality, safety, and staff experience.
































![Organizational Structure Of A Hospital[1]](https://cdn.slidesharecdn.com/ss_thumbnails/organizationalstructureofahospital1-100104091259-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


![Microsystem analysis webinar_feb_21_2013[1]](https://cdn.slidesharecdn.com/ss_thumbnails/microsystemanalysiswebinarfeb2120131-130220151815-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






































