Downloaded 40 times
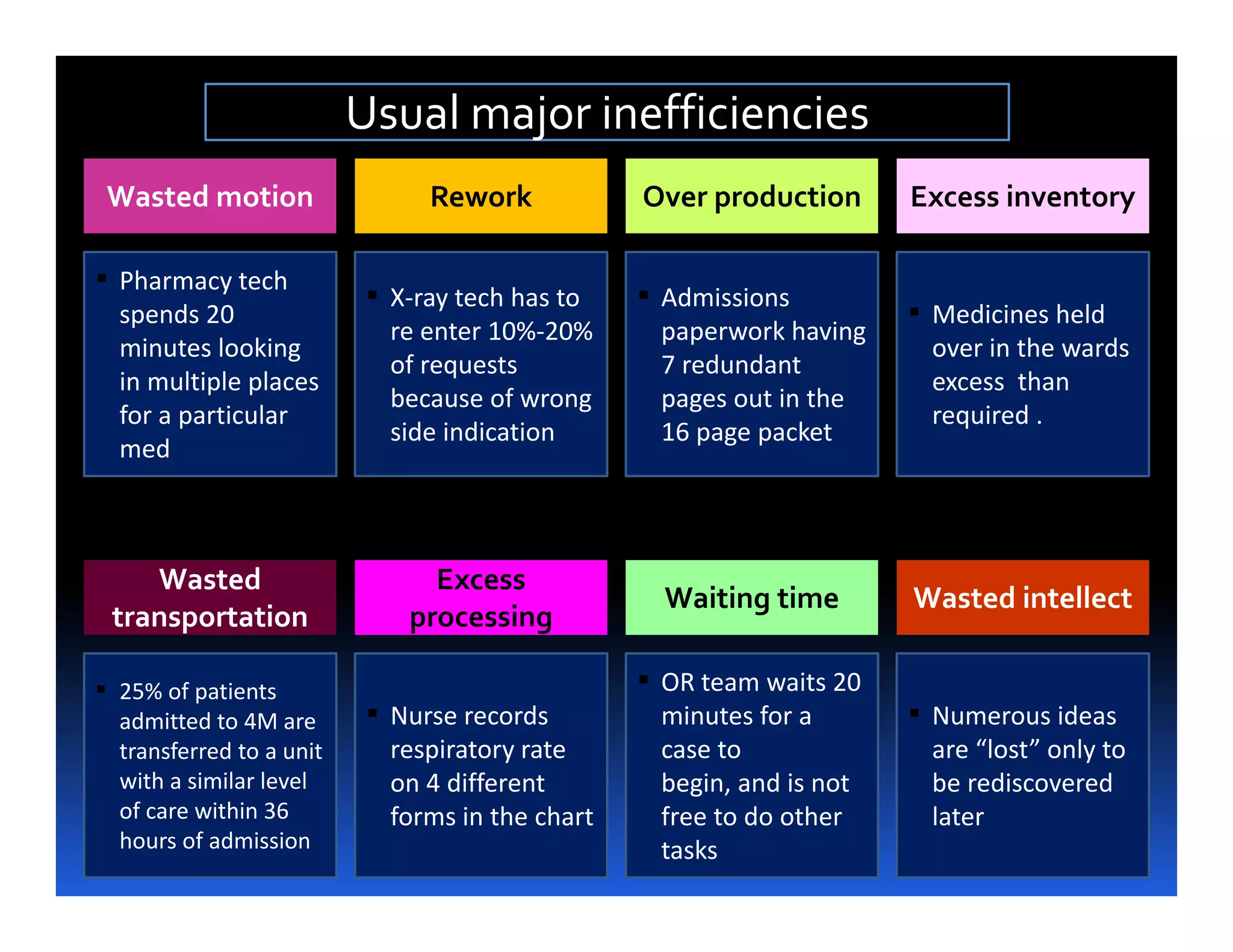
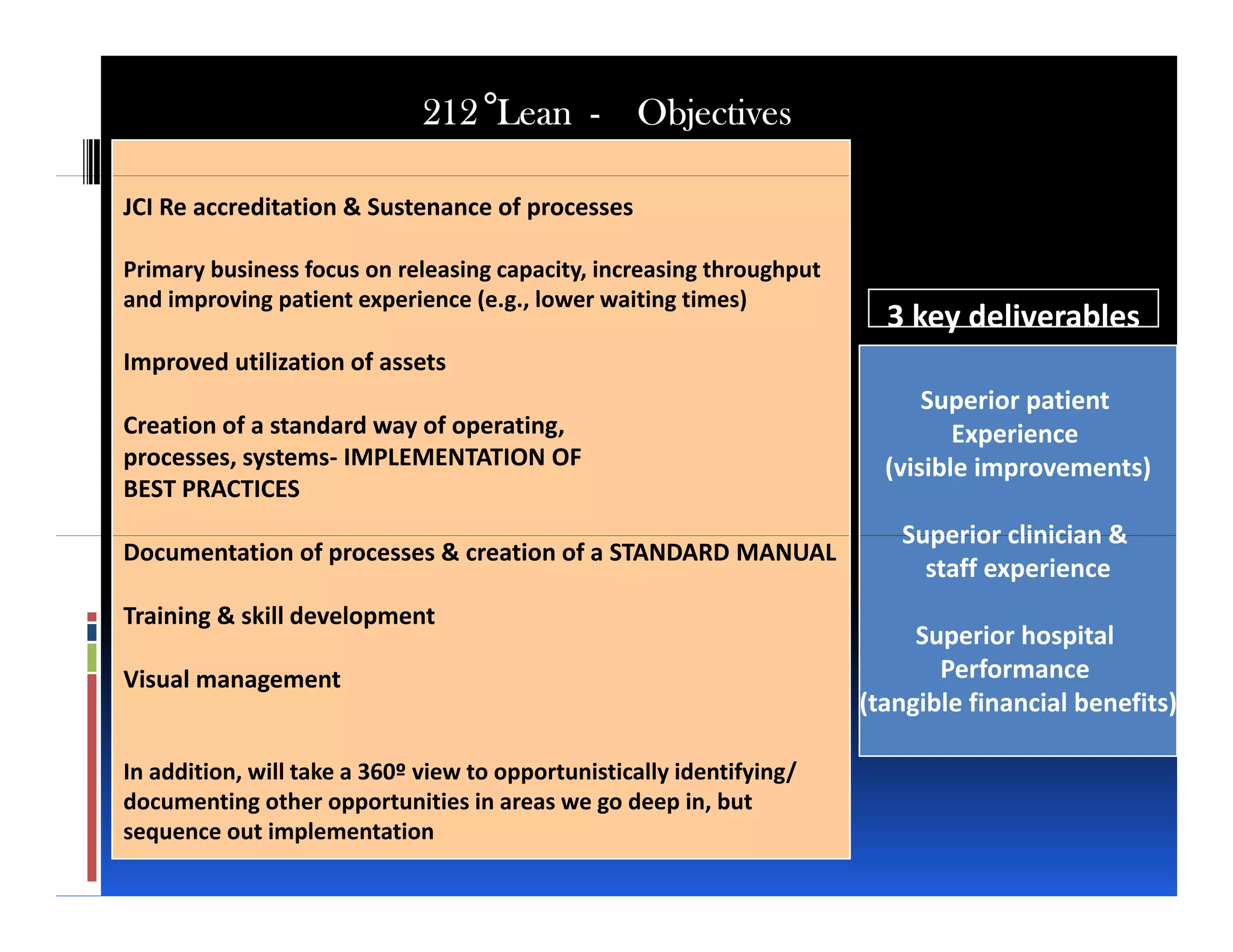
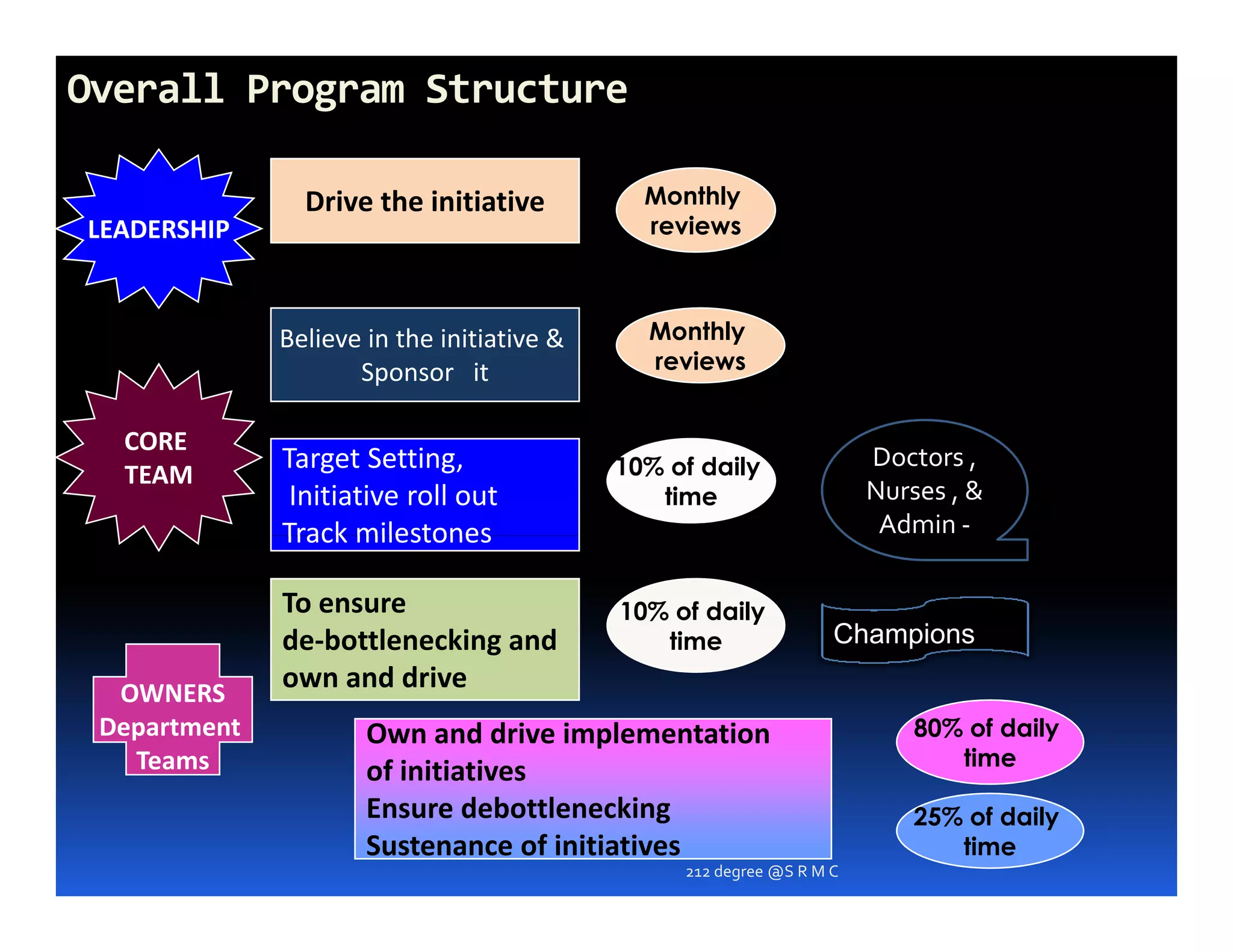
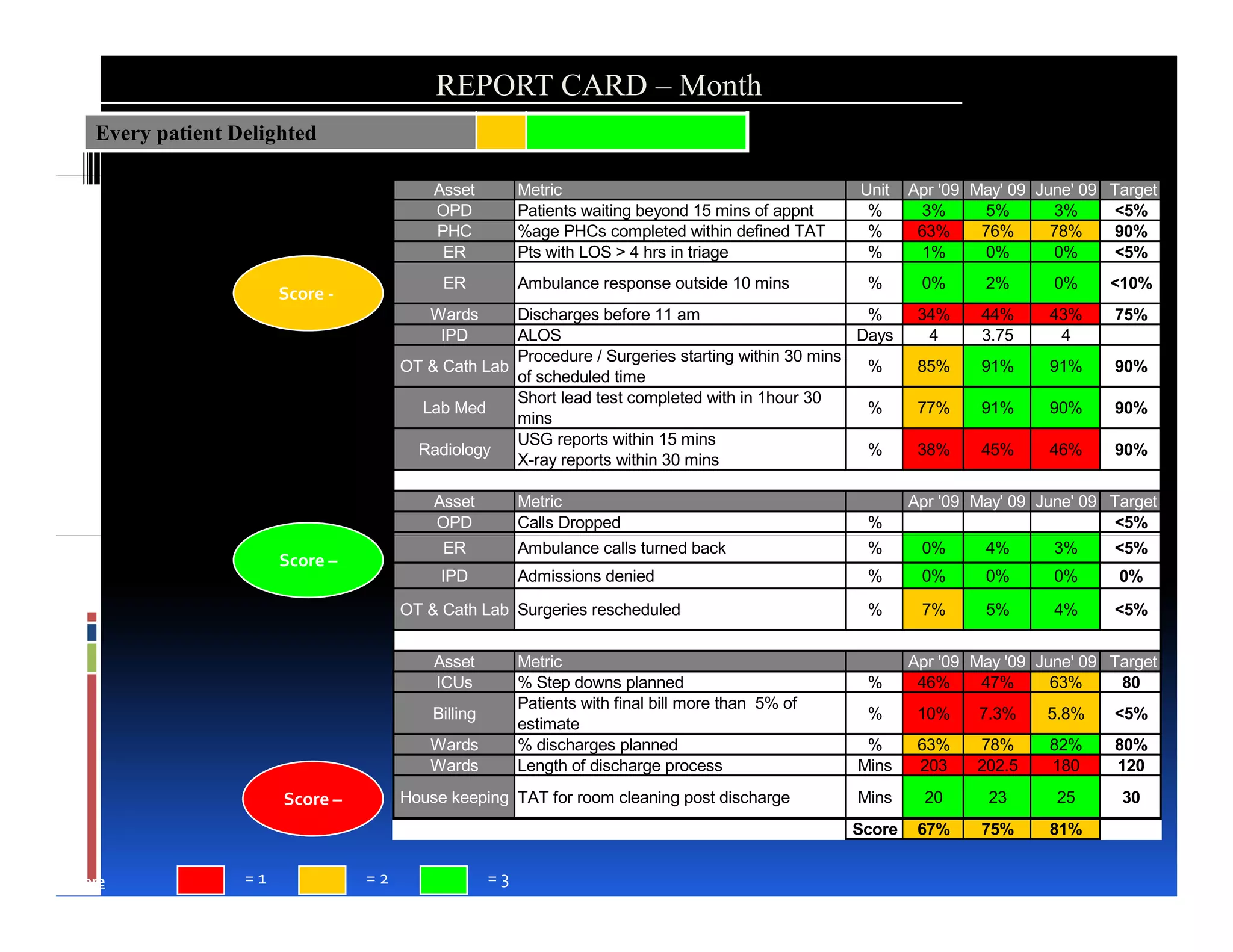






This document discusses implementing lean processes at a hospital to improve performance. It outlines objectives like achieving JCI re-accreditation, increasing throughput, and improving the patient and staff experience. The document describes collecting initial data, identifying bottlenecks, and co-creating solutions. It also outlines establishing leadership support, core and department teams, and implementing best practices to build capacity and sustain initiatives through review and monitoring. The overall aim is to enhance the hospital's operations and service delivery through lean methodology.


















![Delivering care in efficient environment medicall 2011 [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/deliveringcareinefficientenvironment-medicall2011compatibilitymode-110831063224-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




