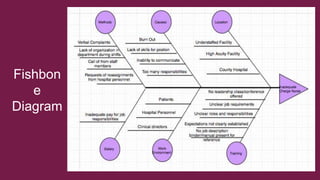
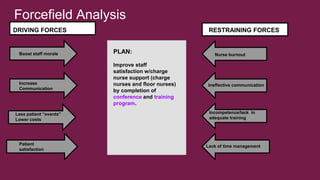
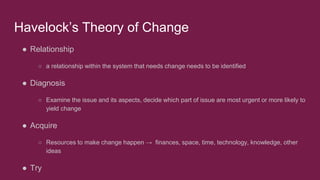
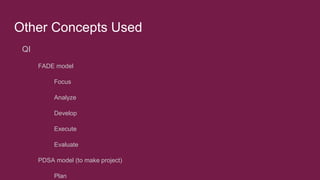
The N.A.C.U. (Nursing Attitude Control Unit) was called in to address complaints about two different charge nurses - Christina and Jamie. Christina was actively involved in patient care and supporting nurses. Jamie stayed in the office all day and provided no support. The N.A.C.U. proposed a training program to improve charge nurse leadership using concepts like the PDSA cycle, force field analysis, and Havelock's theory of change. An evaluation plan included surveys, interviews and reviewing outcomes like HCAHPS scores to assess the impact. The goal was to facilitate positive relationships and decrease burnout by ensuring charge nurses support nurses and patients.





![Literature Review
Crowther (2004) stated that, “The scope of the [charge nurse] is wide-ranging. A
charge nurse manager enters the role with advanced clinical expertise and must
promptly become a:
● Strategic planner
● Human Resource Authority
● Quasi-Business Manager
● Financial Analyst
● Risk Manager
● Operations Manager
In addition, “Charge nurses manage:
● Budgets
● Rosters
● Beds
● Patients
● Families
● Colleagues
● Compliance
● Professional regulatory rules
● Organizational policies
● Procedures
● Quality assurance systems”](https://image.slidesharecdn.com/9974638c-1a38-4878-b247-50626f3b42b6-161130011339/85/Qsen_Change-14-320.jpg)
![Literature Review
● Nurses looking to be promoted to charge nurses should:
○ “[Enroll] in a Post Graduate Diploma in Health Management [to prepare, including] the study of
human resources, accounting, operations management, health management, health
organization, quality in health care and health economics” (McCallin & Frankson, 2010, p.
324).
○ Participate in a training program that emphasizes:
■ “Emotional self-management, relationship management, graduate education,
management training and formal mentoring” (McCallin & Frankson, 2010, p. 324).](https://image.slidesharecdn.com/9974638c-1a38-4878-b247-50626f3b42b6-161130011339/85/Qsen_Change-16-320.jpg)
![Literature Review
● Incorporating reflection coping strategies
○ “Could help [nurses] to become more introspective and consequently respond more
constructively to their own needs, promoting wellbeing and reducing the risk of burnout”
(Fearon & Nicol, 2011, p. 39).
■ 34% of hospital staff nurses reported being burned out
■ 16% of nonclinical pharmaceutical staff reported being burned out (McHugh, Kutney-Lee, Cimiotti,
Sloane, & Aiken, 2011, para. 31).
○ Teaching and spreading positivity among staff
○ Charge nurses should focus on “[appreciating] the contributions of the employees [...] and](https://image.slidesharecdn.com/9974638c-1a38-4878-b247-50626f3b42b6-161130011339/85/Qsen_Change-18-320.jpg)

![References:
❖ Duygulu, S., & Kublay, G. (2011). Transformational leadership training programme for charge nurses. Journal Of Advanced Nursing, 67(3), 633-642.
doi:10.1111/j.1365-2648.2010.05507.
❖ Duke University. (2016). Patient Safety: Quality Improvement. Retrieved from: http://patientsafetyed.duhs.duke.edu/index.html
❖ Fearon, C., & Nicol, M. (2011). Strategies to assist prevention of burnout in nursing staff. Nursing Standard, 26(14), 35-39.
❖ Havelock, R. (1995). The Change Agent’s Guide. [DX Reader Version]. Retrieved from https://books.google.com/books?hl=en&lr=&id=h-
uIrSJeVyUC&oi=fnd&pg=PR5&dq=Havelock++R+(1995)++The++Change++Agent%27s++Guide.&ots=n5ypBdF4x6&sig=NlMbaNIbpVmMpH5J2EPsHieJV
N4#v=onepage&q&f=false
❖ McCallin, A., & Frankson, C. (2010). The role of the charge nurse manager: a descriptive exploratory study. Journal Of Nursing Management, 18(3), 319-
325. doi:10.1111/j.1365-2834.2010.01067.
❖ McHugh, M. D., Kutney-Lee, A., Cimiotti, J. P., Sloane, D. M., & Aiken, L. H. (2011). Nurses’ widespread job dissatisfaction, burnout, and
frustration with health benefits signal problems for patient care. Health Affairs (Project Hope), 30(2), 202–210.
http://doi.org/10.1377/hlthaff.2010.0100
❖ Platt, J., & Foster, D. (2008). Revitalizing the charge nurse role through a bespoke development programme. Journal Of Nursing Management, 16(7), 853-
857. doi:10.1111/j.1365-2834.2008.00939
❖ Snow, T. (2012). Trusts take ‘cheap option’ and use inexperienced staff to run wards. Nursing Standard, 27(10), 11.](https://image.slidesharecdn.com/9974638c-1a38-4878-b247-50626f3b42b6-161130011339/85/Qsen_Change-27-320.jpg)














































