Download as PDF, PPTX

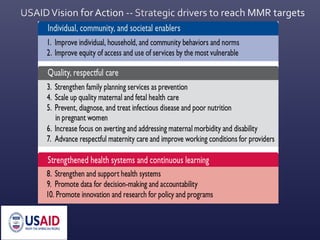


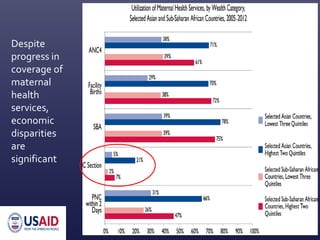

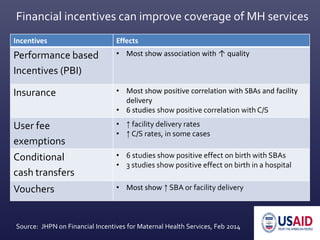
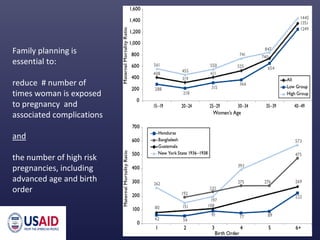
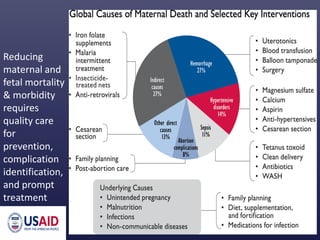
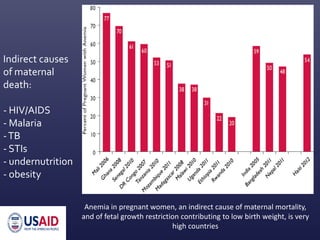


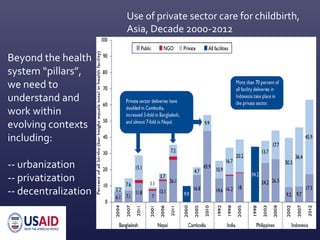
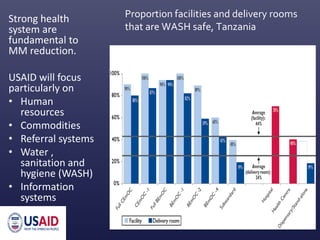
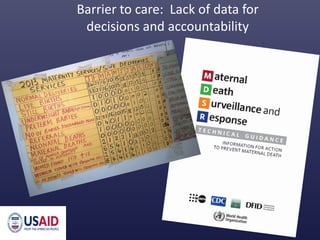

This document summarizes USAID's Maternal Health Vision for Action plan to end preventable maternal mortality globally by 2030. The plan focuses on 10 key strategies: 1) improving individual and community behaviors, 2) increasing access to services for vulnerable groups, 3) integrating family planning and maternal services, 4) scaling quality maternal/fetal care, 5) treating indirect causes of mortality, 6) addressing morbidity, 7) respectful maternity care, 8) strengthening health systems, 9) using data for decisions, and 10) promoting innovation. Financial incentives, community mobilization, addressing disparities, and strengthening health systems are emphasized as ways to achieve the vision.