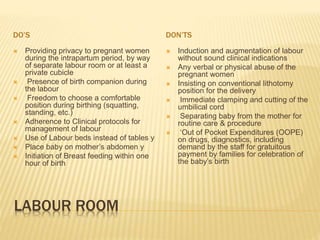
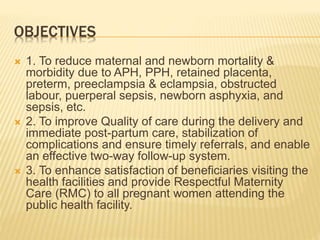
The Laqshya programme, initiated in Karnataka in 2018-19, aims to improve quality in maternity care by reducing maternal and newborn mortality and enhancing respectful maternity practices. Key objectives include achieving high patient satisfaction, ensuring adherence to clinical protocols, and enhancing the overall quality of labor rooms and operating theaters. The initiative also emphasizes training, structural improvements, and systematic monitoring to foster better health outcomes and management of complications during childbirth.





































![Qualityy_improvement_Cycle_1_&_2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/qualityimprovementcycle121-260120083320-8645ffcf-thumbnail.jpg?width=640&height=640&fit=bounds)























![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




