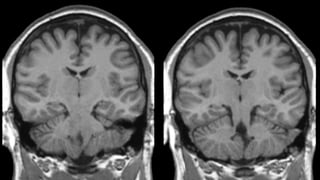
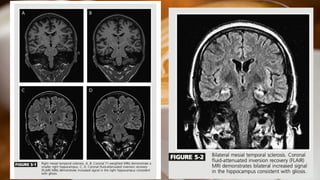
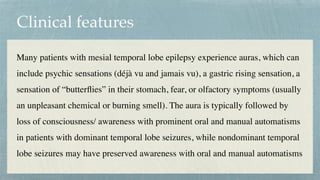
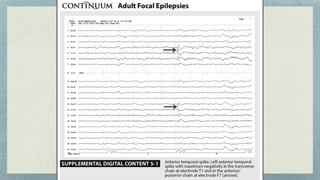
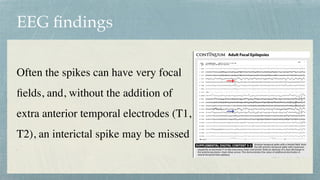
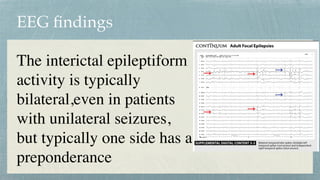
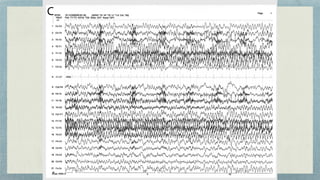
This document discusses mesial temporal sclerosis, a common cause of temporal lobe epilepsy. It presents a case of a 23-year old woman with intractable seizures beginning with an odd smell and staring spells. Mesial temporal lobe epilepsy often begins in late adolescence/early adulthood and can be caused by hippocampal sclerosis or other lesions. Clinical features include auras and seizures characterized by automatisms or dystonic posturing localized to the affected temporal lobe. EEGs show interictal temporal spikes maximum over the affected side while ictal patterns involve rhythmic activity spreading within and between temporal lobes. MRI is used to identify hippocampal sclerosis or other lesions as the cause of seizures.





















































![mts[1] the important cause of epilepsy.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mts1-250410163942-19d8a3ca-thumbnail.jpg?width=640&height=640&fit=bounds)





![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















