Downloaded 54 times

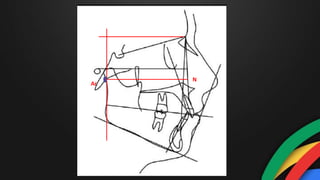
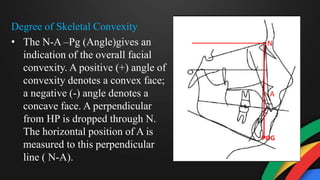
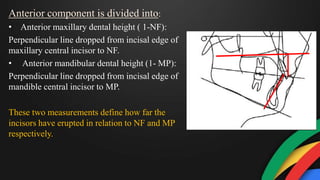
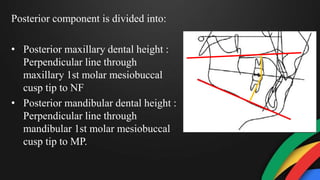
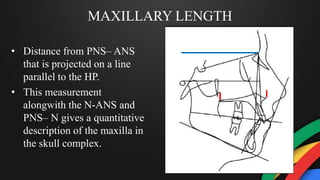
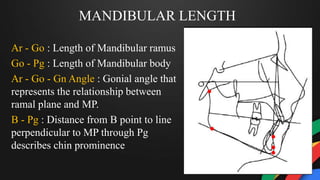

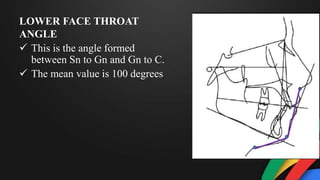
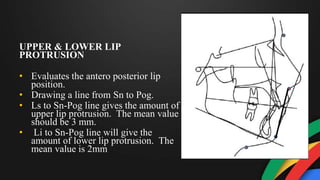
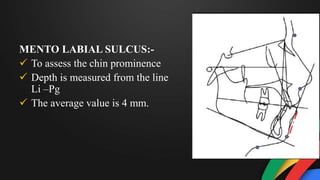
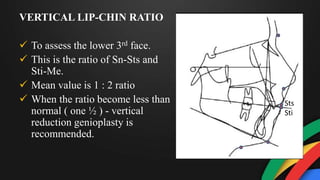
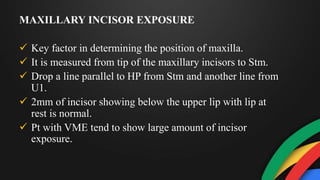

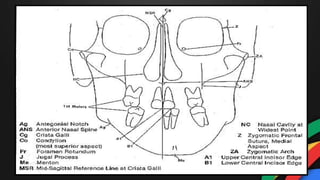

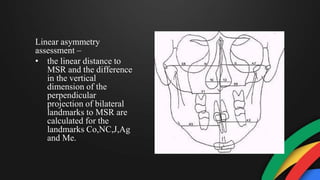
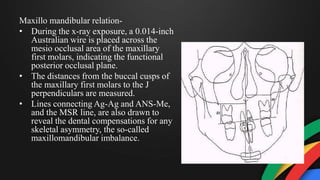
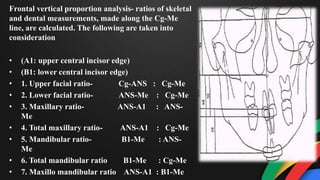
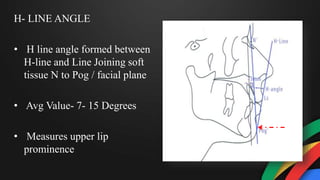

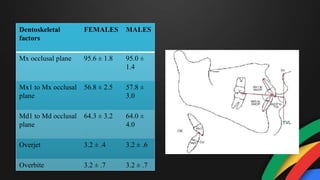
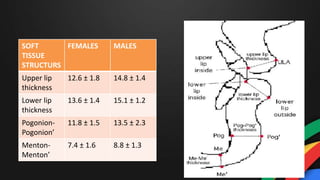
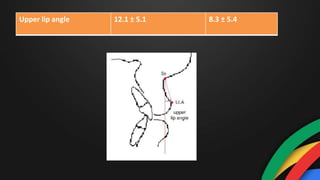

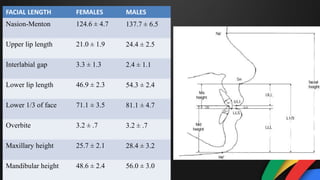
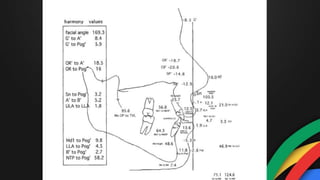


This document discusses various cephalometric analyses used in orthognathic surgery planning, including COGS, Grummons, Holdaway, and Arnett/Bregman analyses. It provides details on landmarks, measurements, and norms for assessing the horizontal and vertical skeletal relationships, dental parameters, and soft tissue profiles. The COGS analysis measures cranial base, maxilla, mandible, occlusal plane and dental angulations. Norms are compared to a sample from the University of Colorado. Analysis of cephalometrics is discussed for determining applicable norms for the Rajasthani population in India.









































































