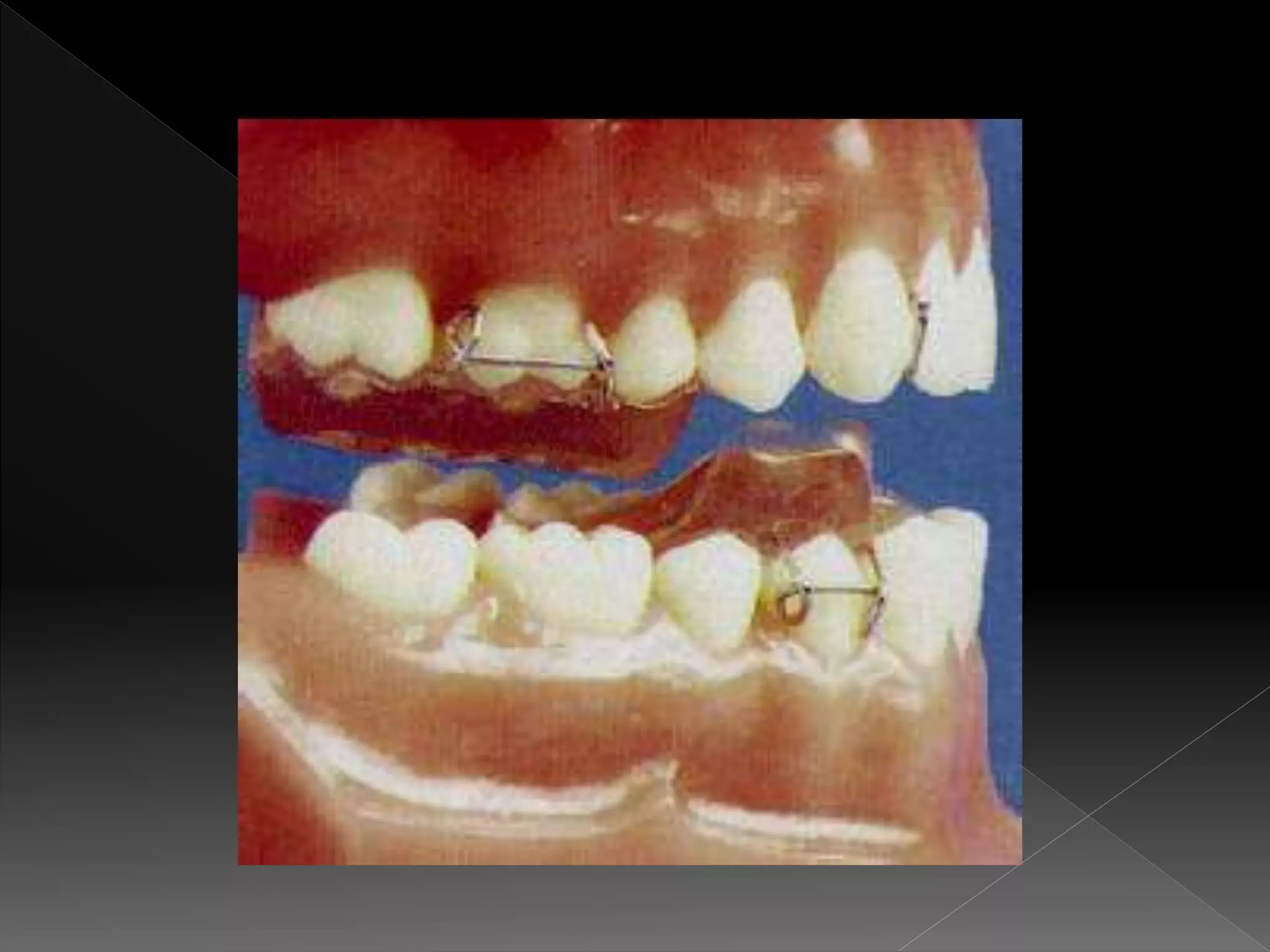
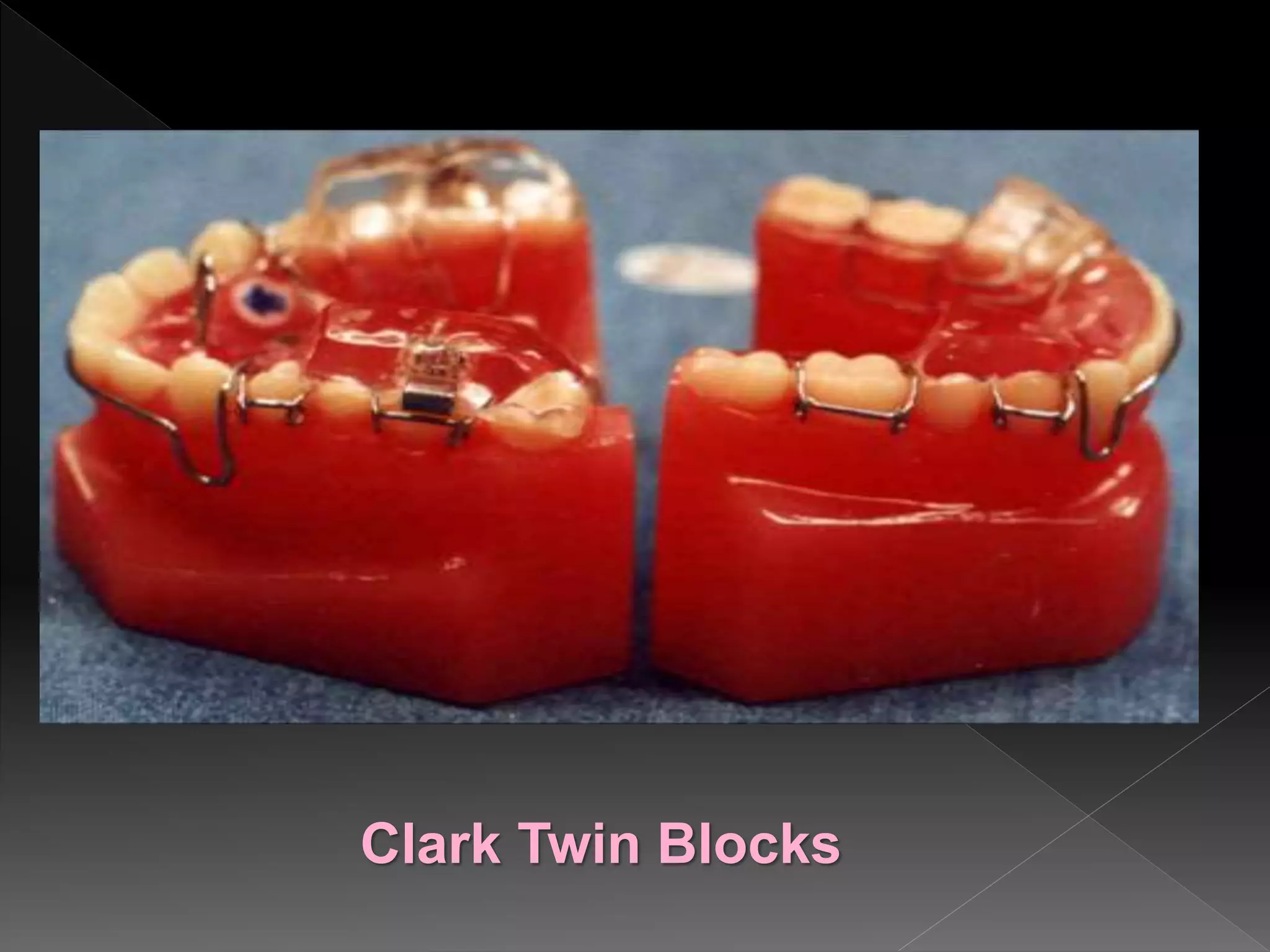
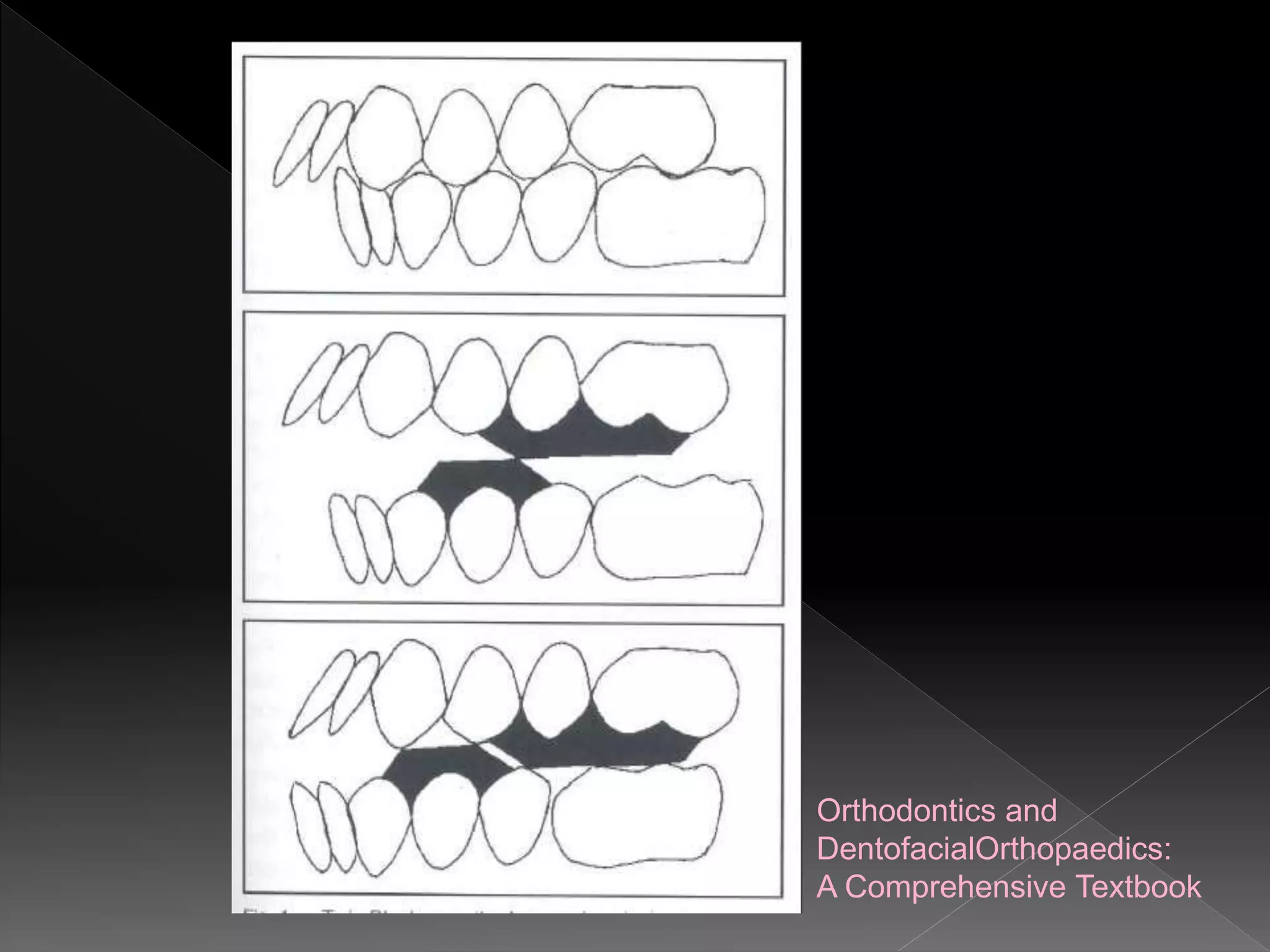
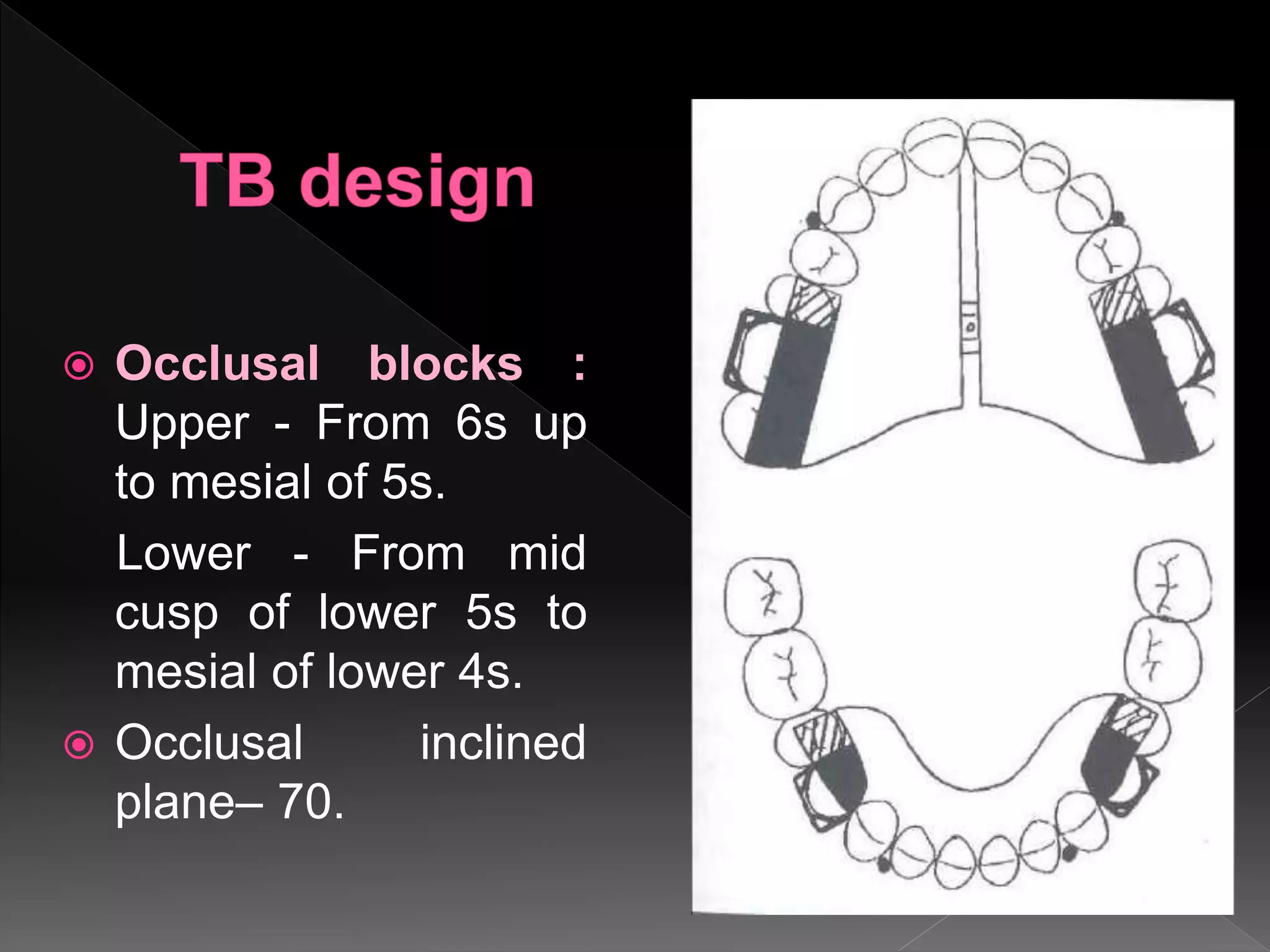
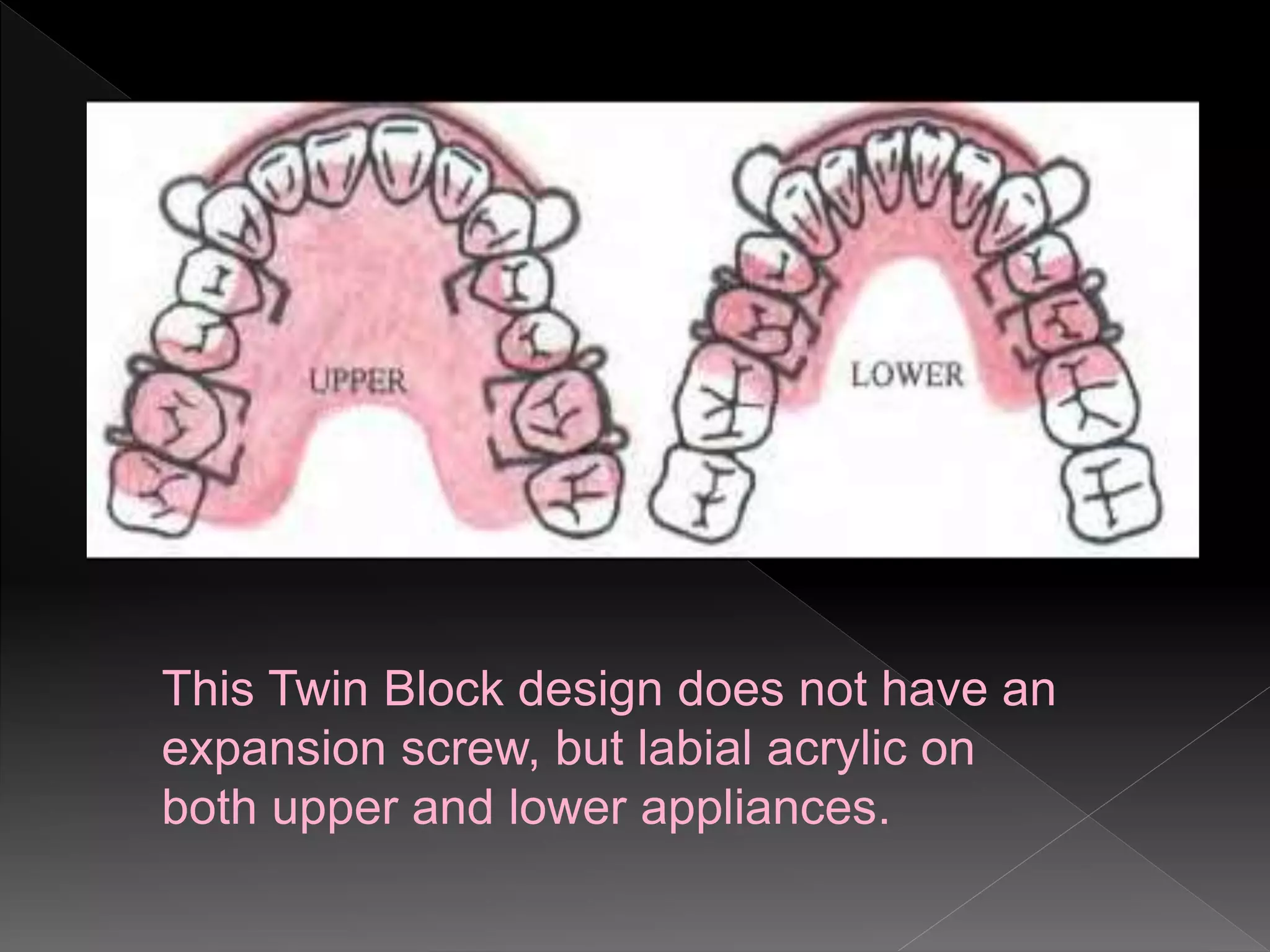
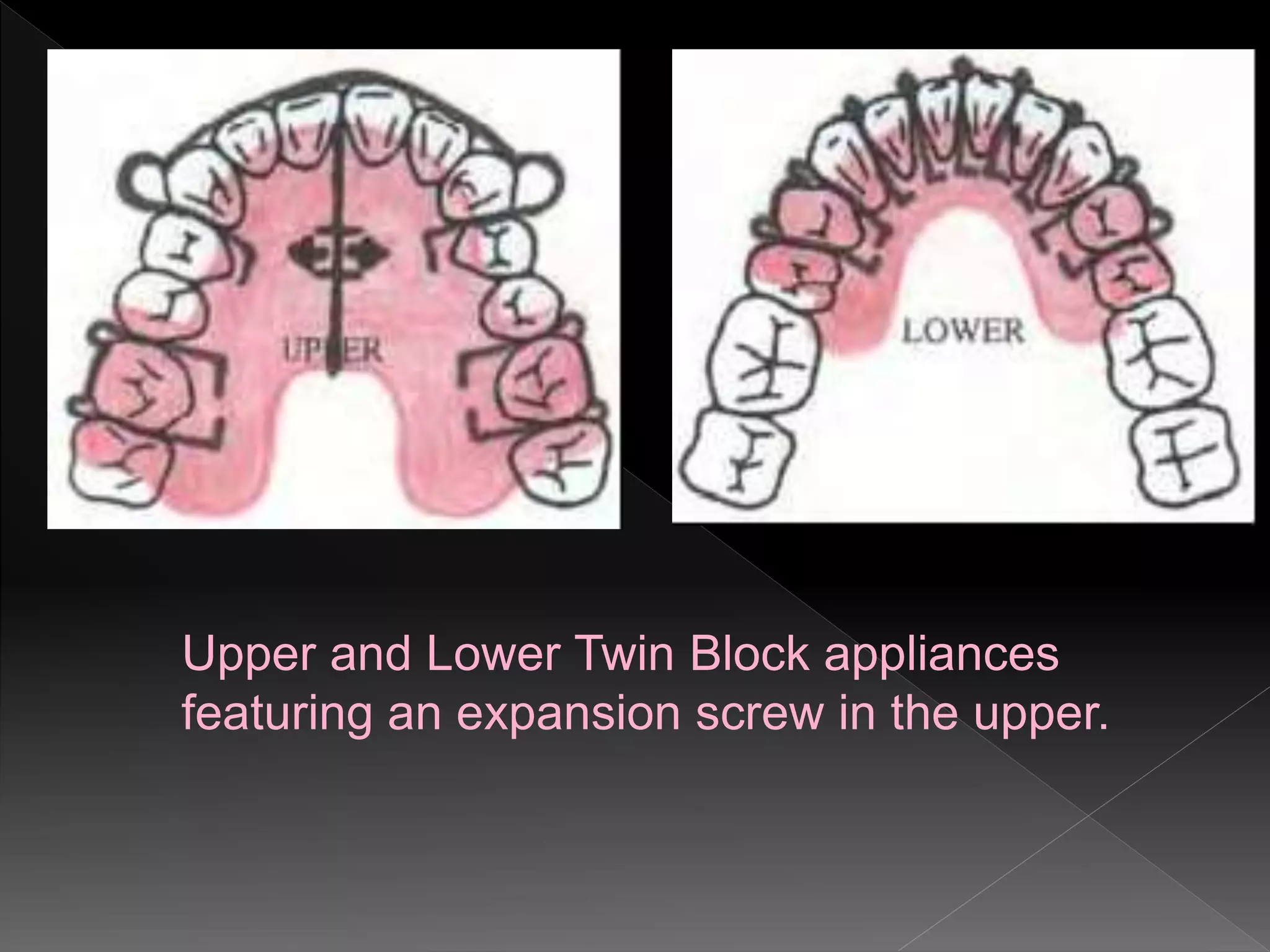
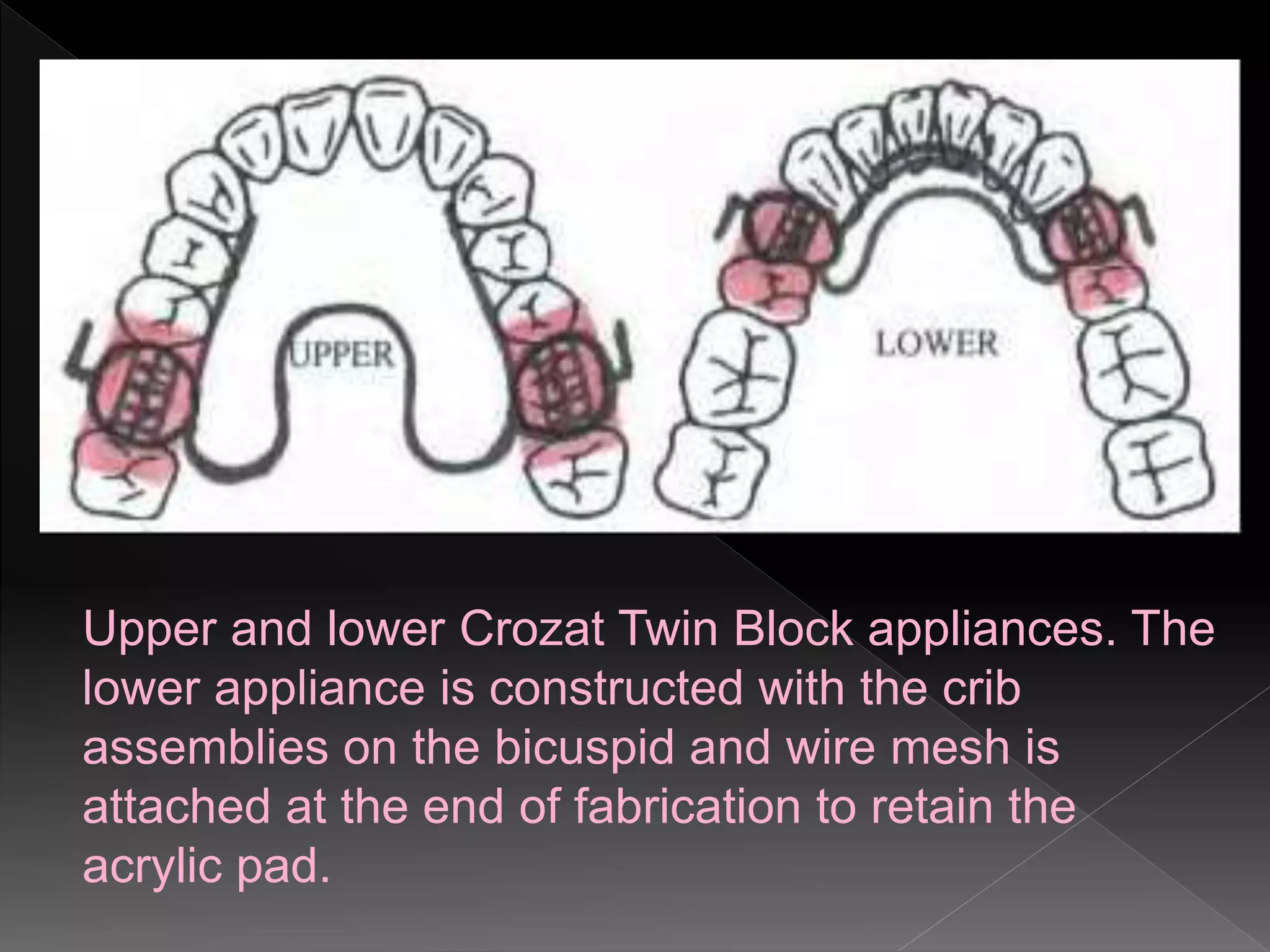
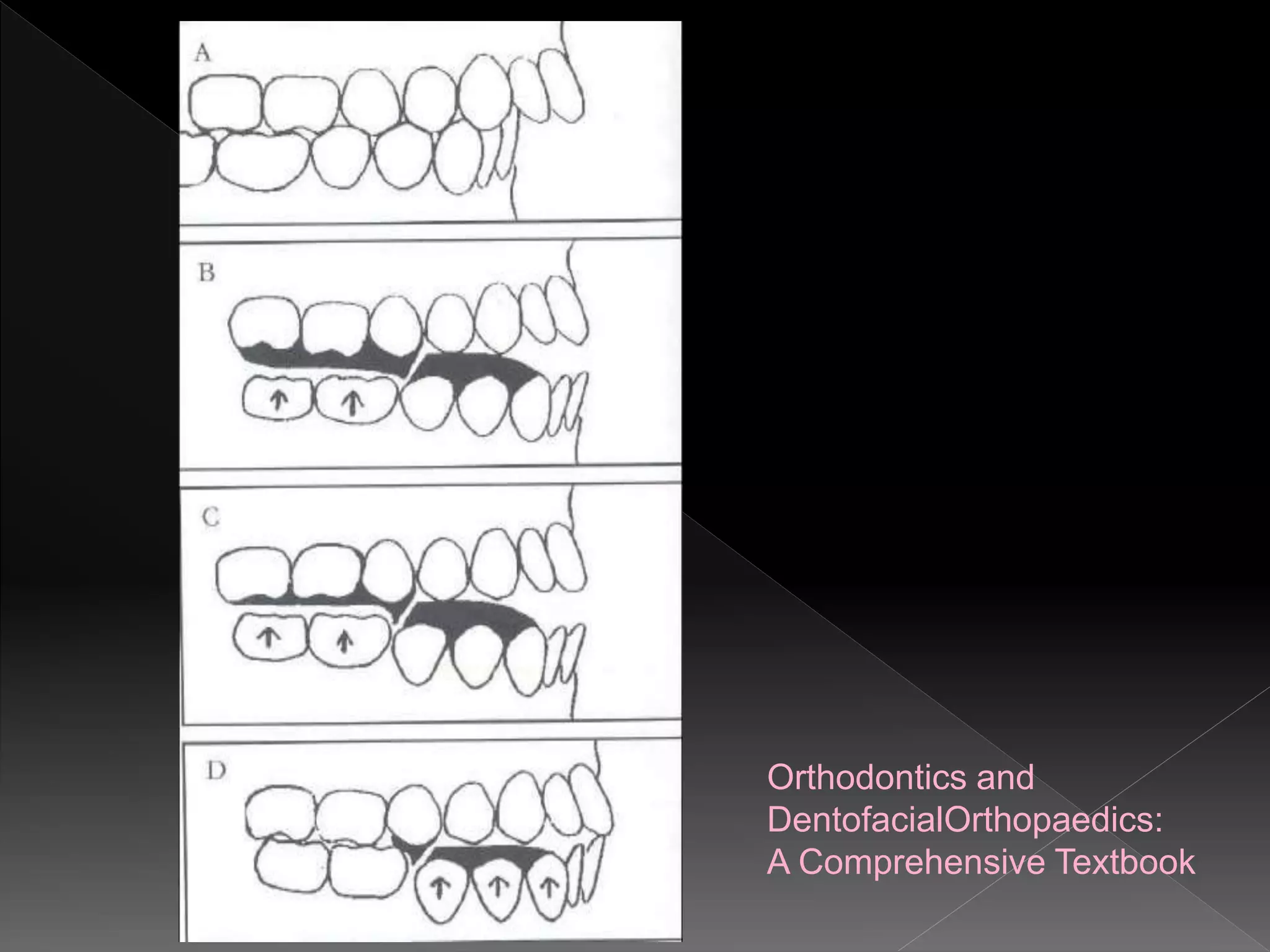
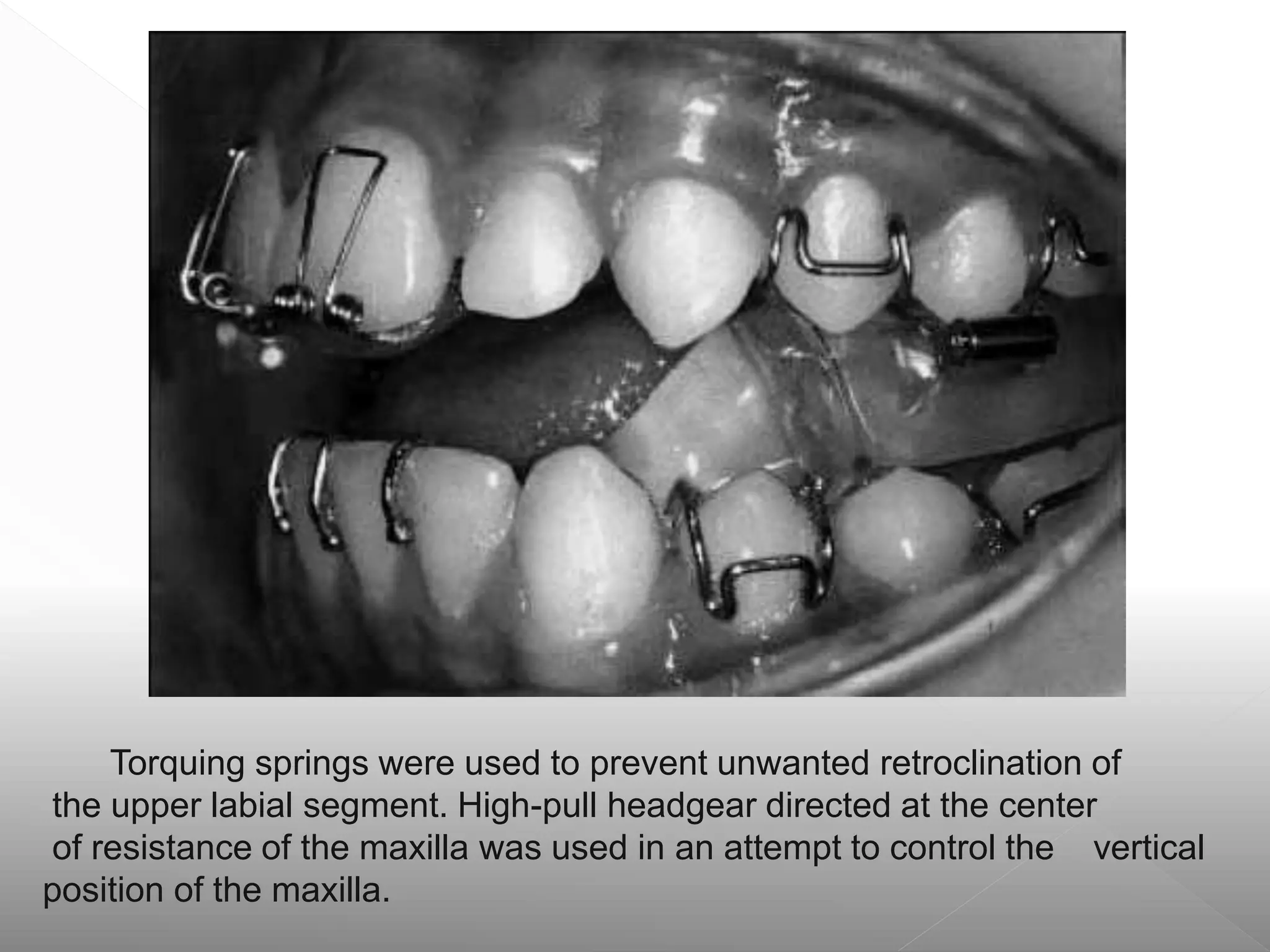
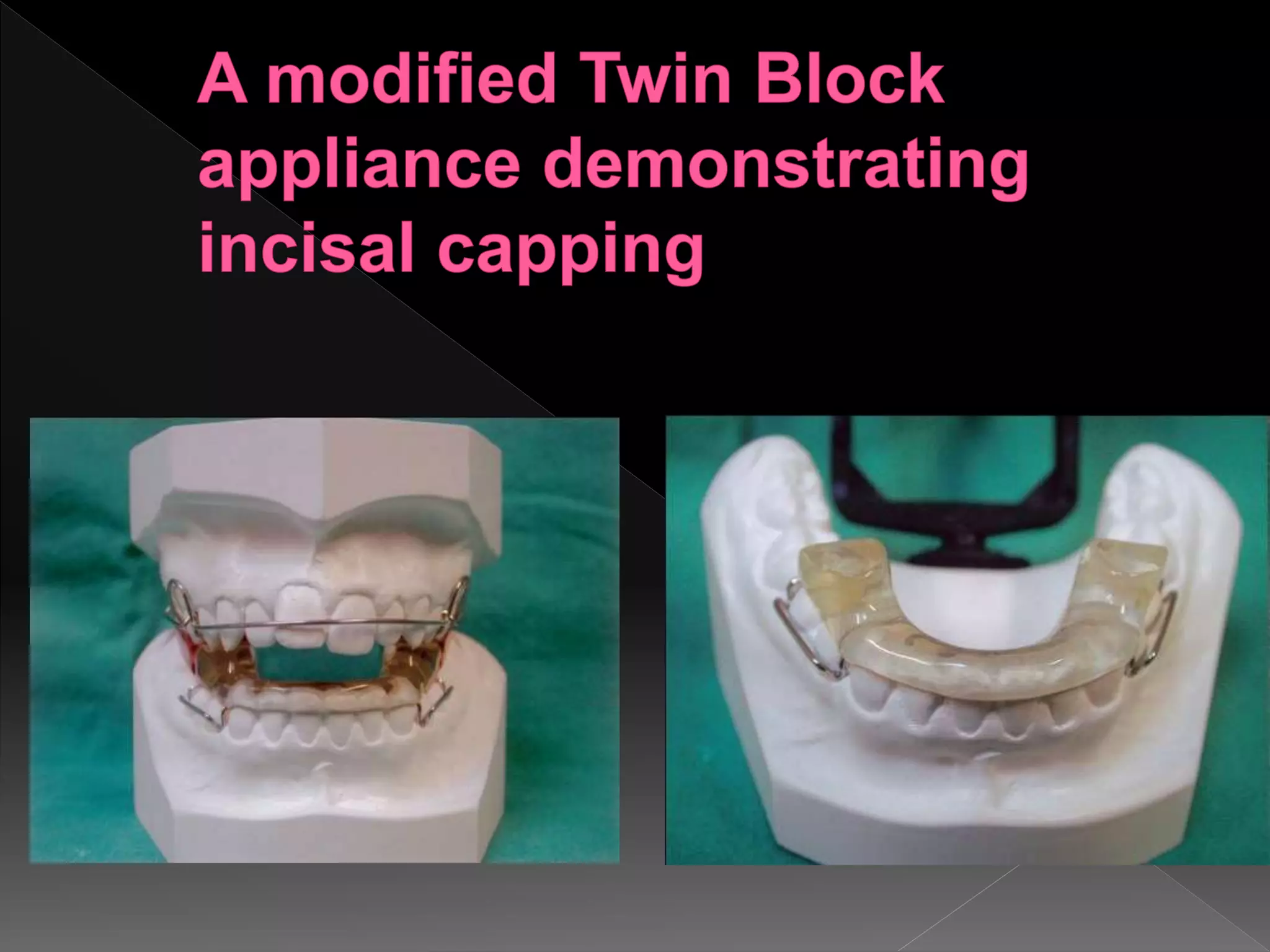
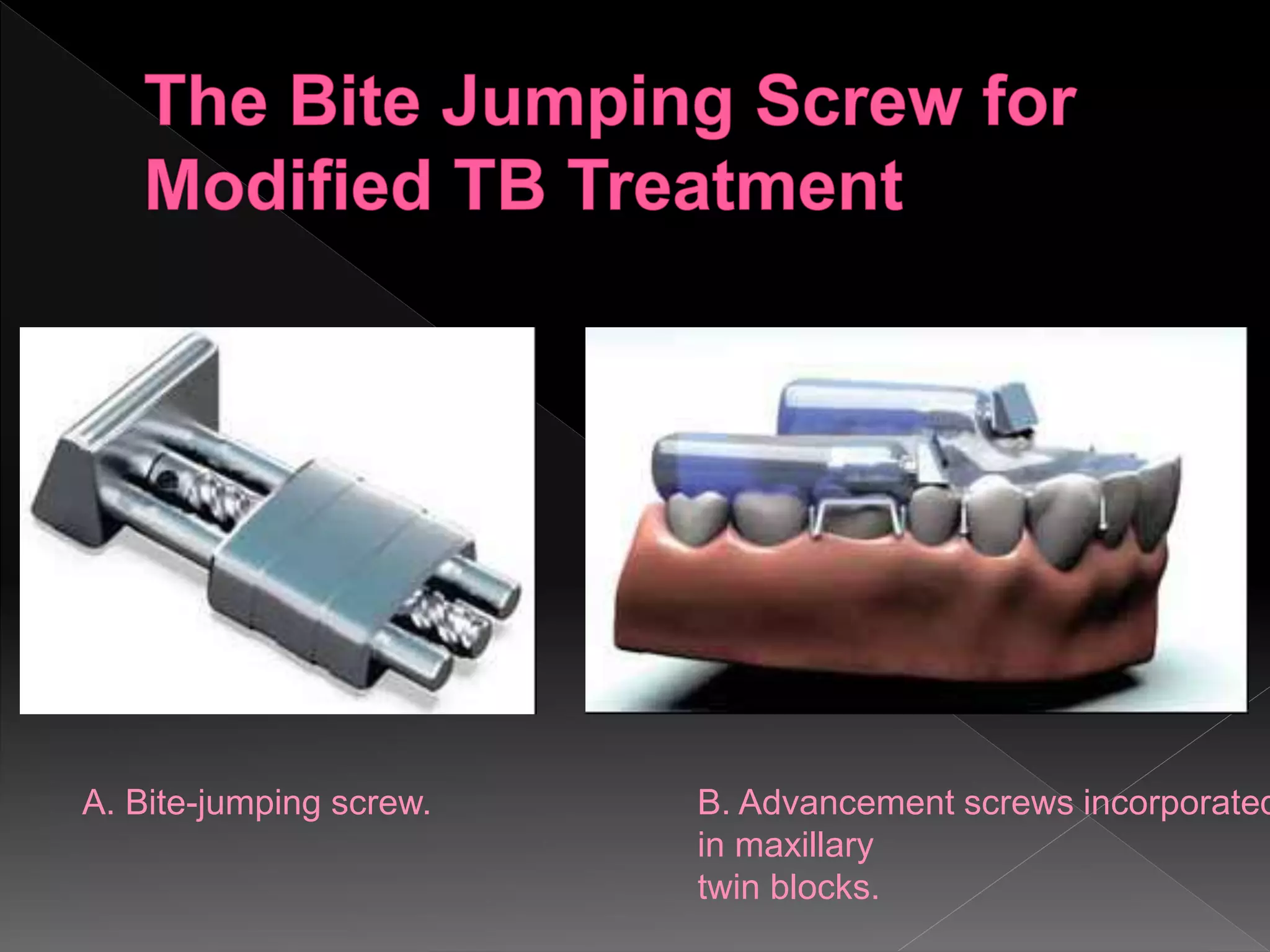
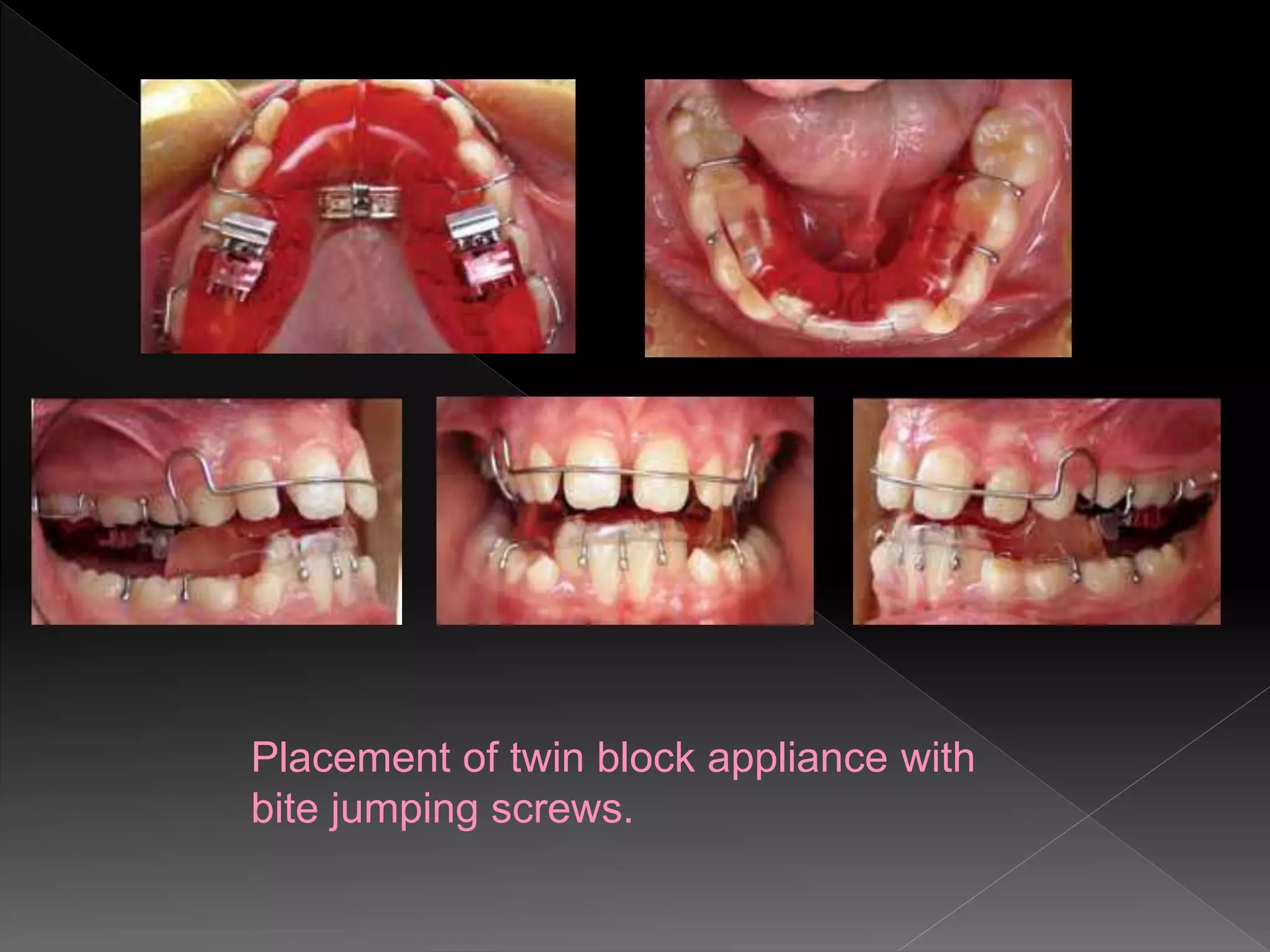
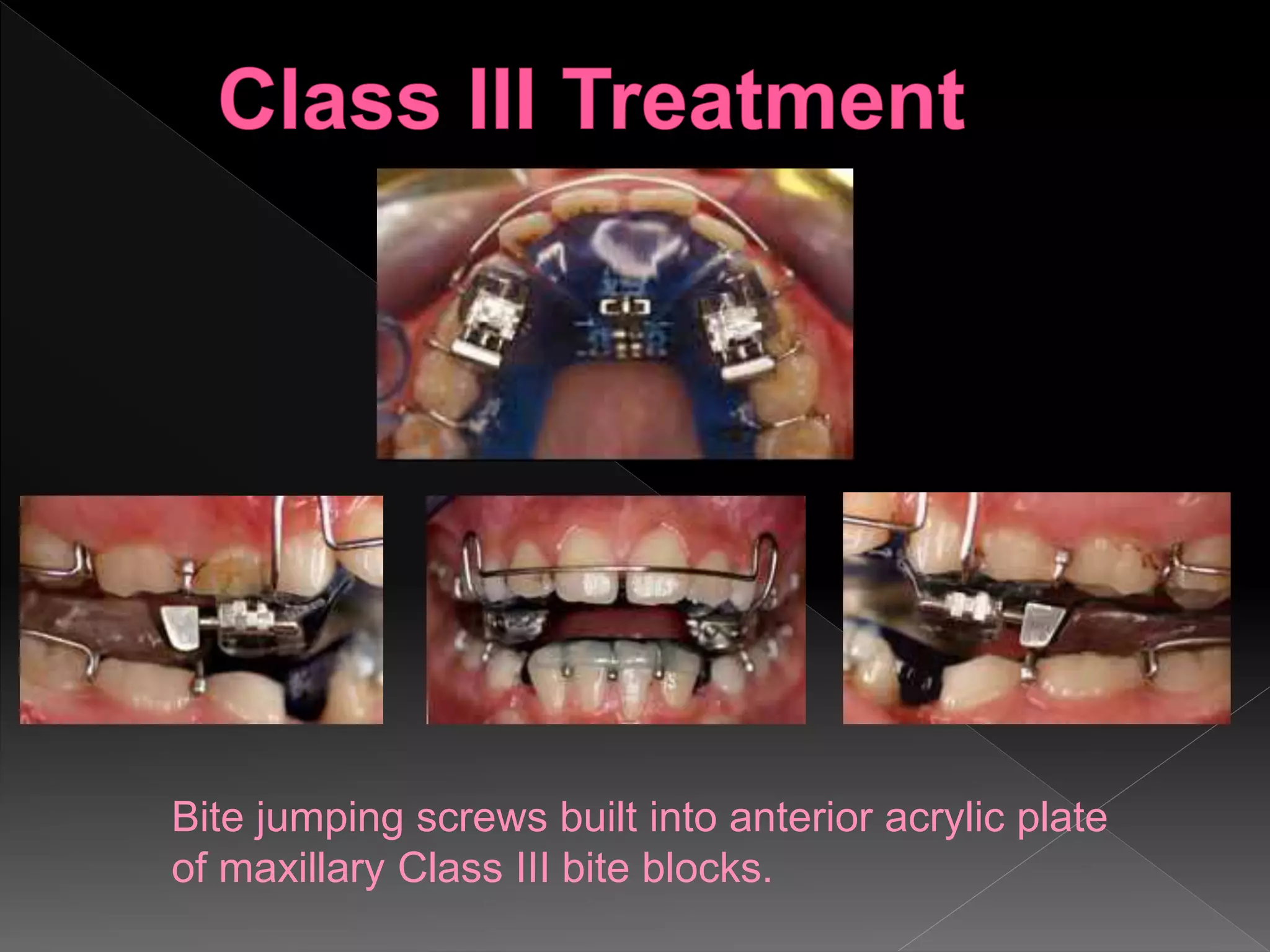
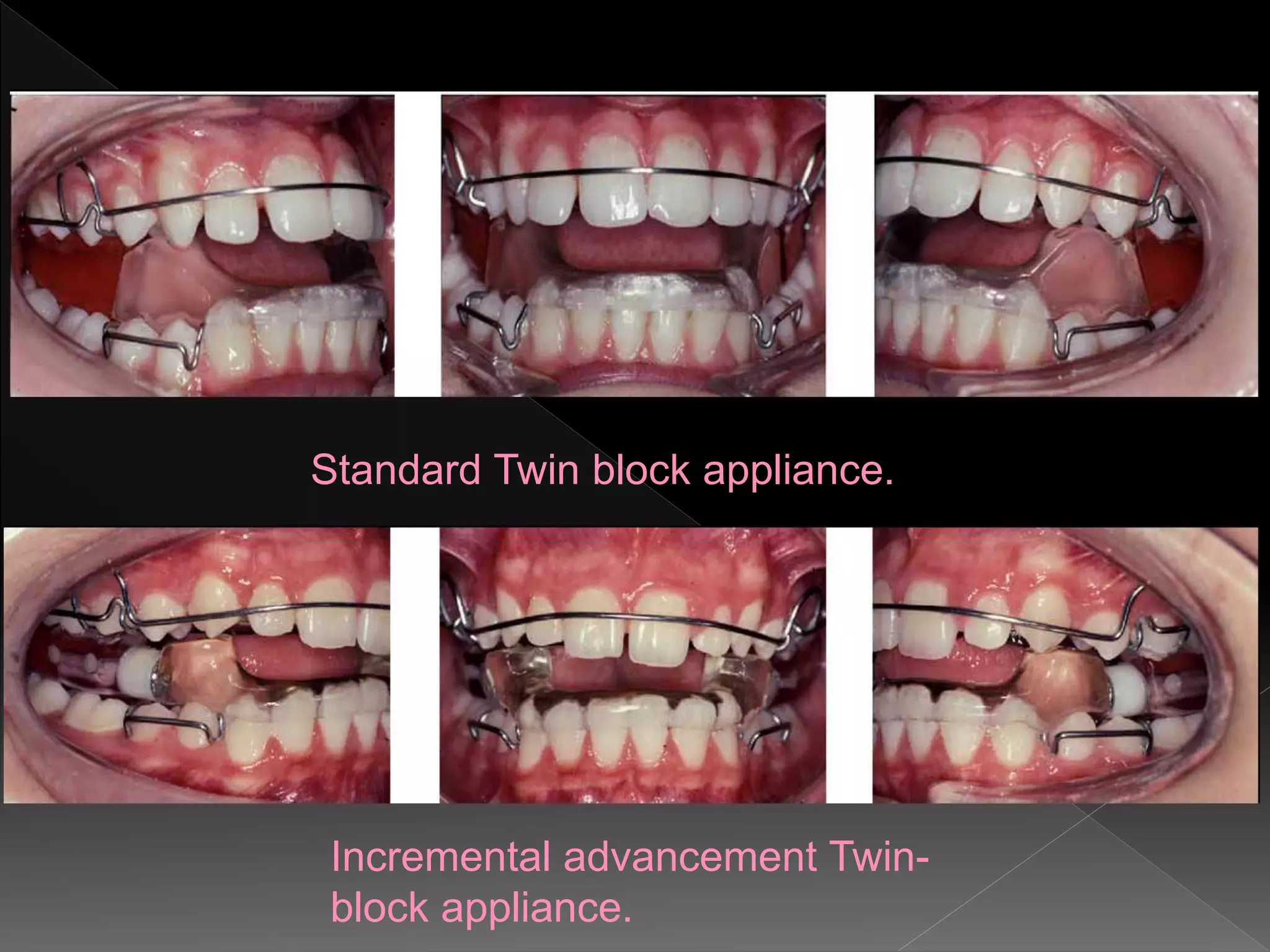
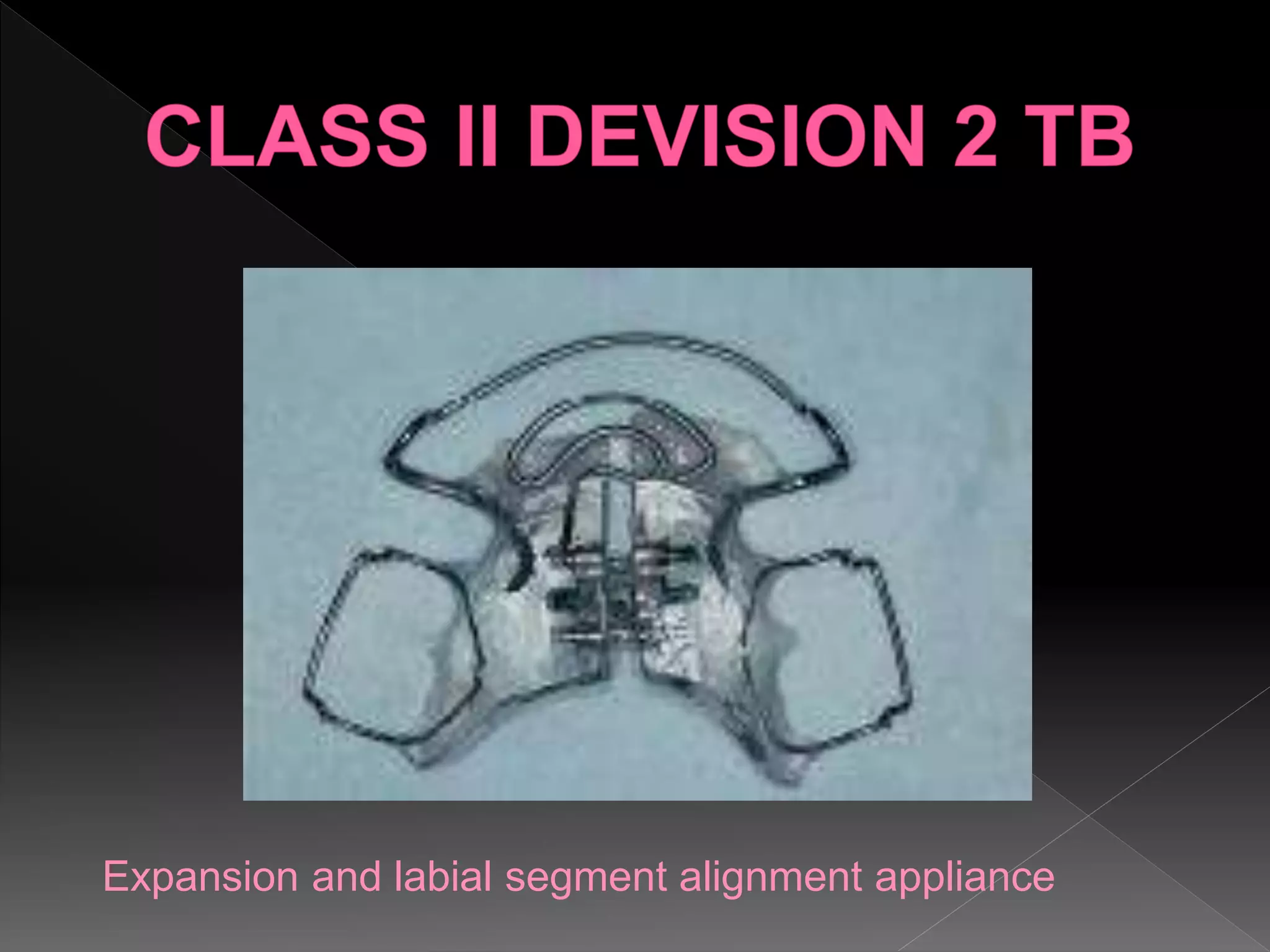
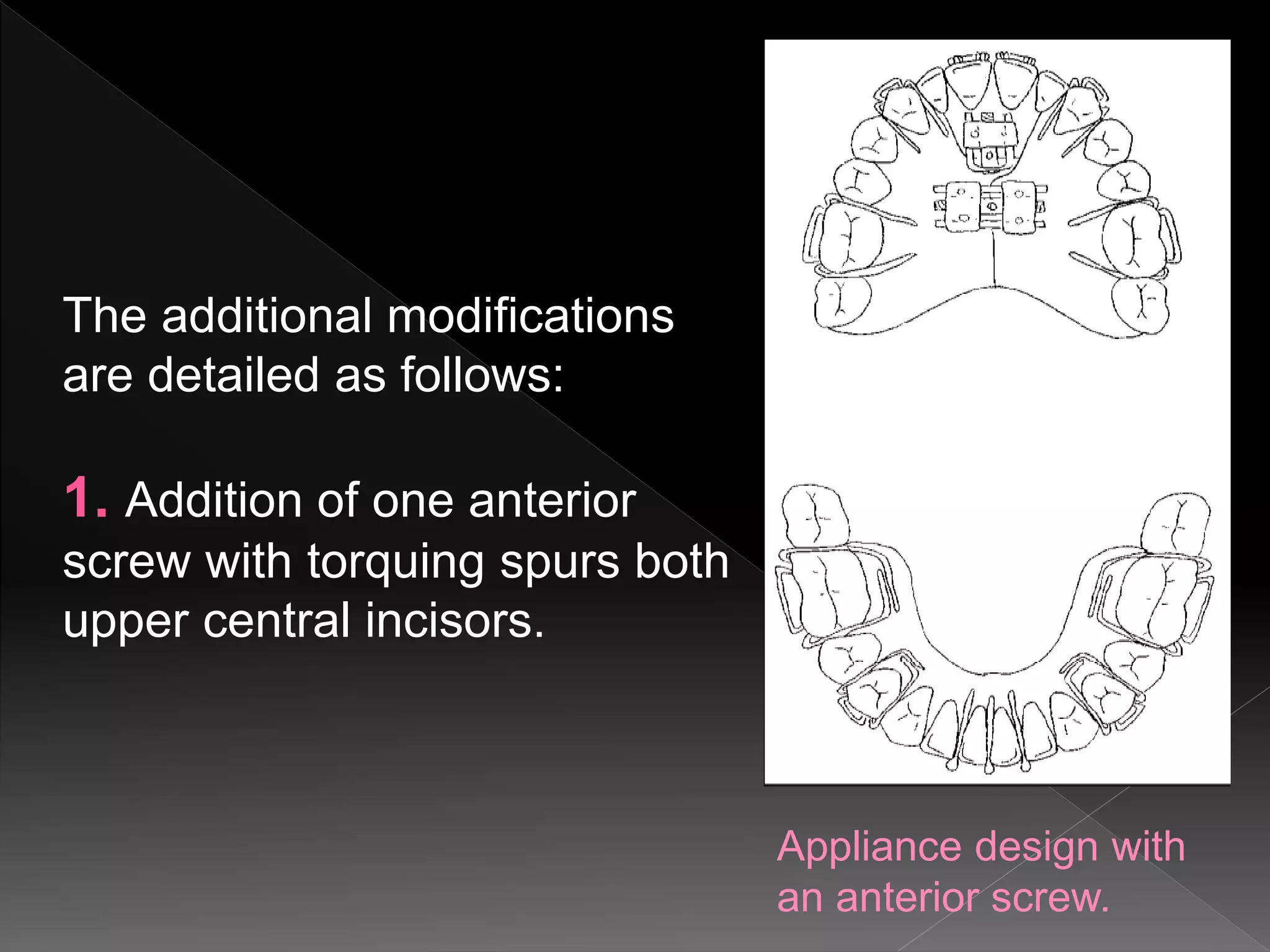
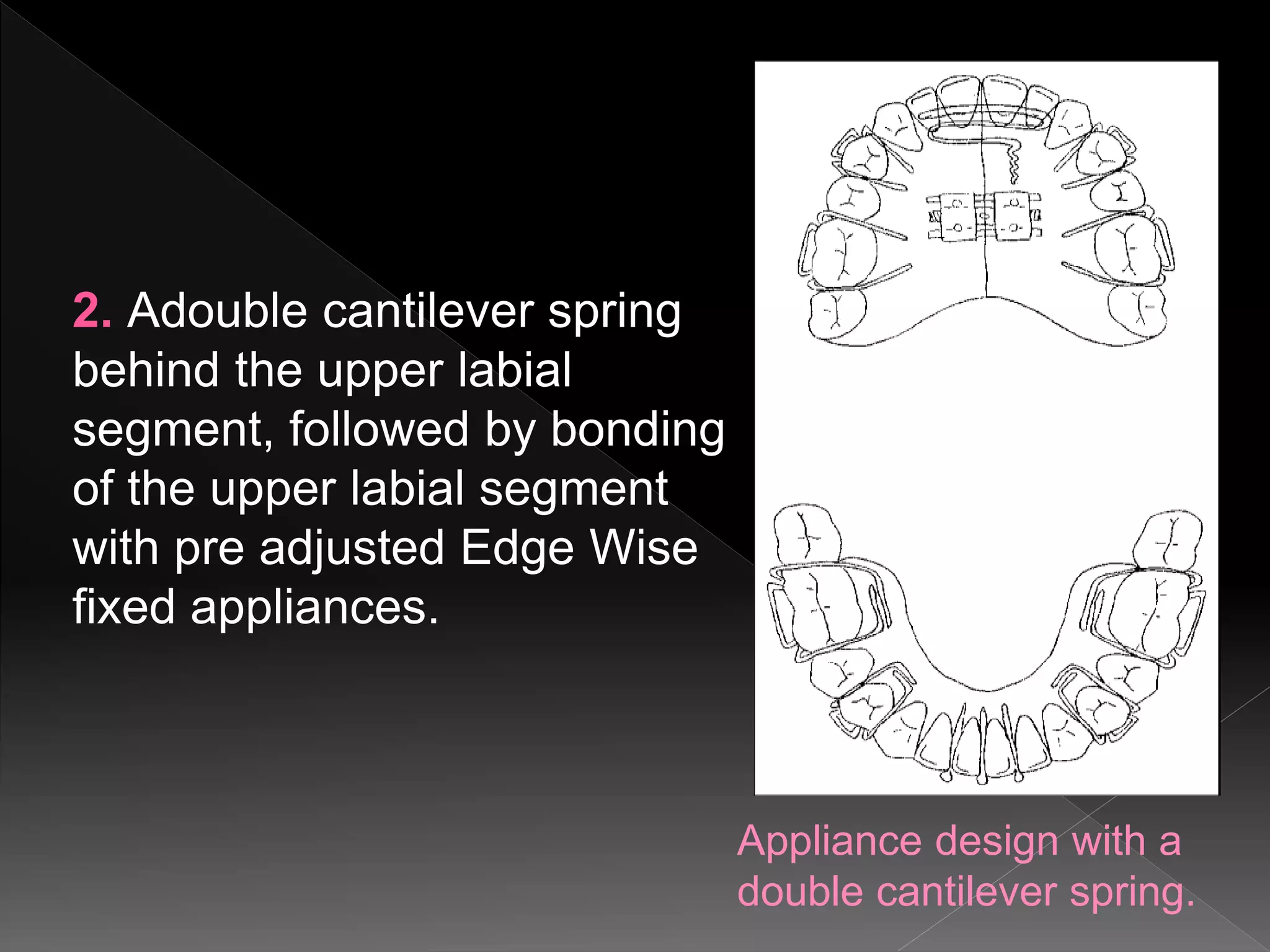
This document discusses the Twin Block appliance, which was originally developed by Clarke. It remains a widely used functional appliance for treating Class II malocclusions. The Twin Block consists of separate upper and lower acrylic appliances connected by occlusal blocks. It works by forcing the mandible into a protrusive position during jaw closure. The document describes the standard Twin Block design and various modifications that have been made, including the addition of expansion screws, torquing springs, and bite jumping screws to allow for gradual advancement. Advantages include comfort, aesthetics, and improved patient compliance compared to fixed appliances. The Twin Block is effective at correcting Class II malocclusions in a rapid manner.