Download as PDF, PPTX
![• Few malocclusions except socioeconomic parameters
were associated with TMD signs, and these associations
i t d ith i d th i ti
were mostly weak.
• Only bilateral open bite up to 3 mm appeared to be
clinically relevant and was associated with TMD signs
(
(odds ratio [OR] = 4.0). This malocclusion, however,
[ ] ) , ,
was of rare occurrence, with a prevalence of 0.3% (n =
9).
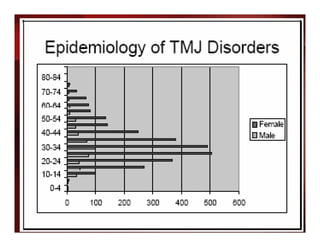
Sample size of 4310 men and women aged 20 to 81 years
(response 68.8%) was investigated for TMD signs, malocclusions,
functional occlusion factors, and sociodemographic parameters
using multiple logistic regression analysis
Gesch et al., Angle Orthod. 2004 Aug;74(4):512-20](https://image.slidesharecdn.com/tmjortho-130411041826-phpapp01/85/Tmj-ortho-34-320.jpg)
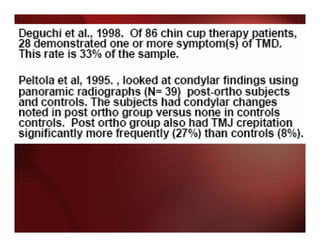




The document discusses temporomandibular joint disorders (TMD) and their relationship to orthodontic treatment. Some key points: - TMD signs and symptoms are common in the general population and usually increase with age, unrelated to orthodontic treatment. - Orthodontic treatment does not increase or decrease the risk of developing TMD. No specific orthodontic mechanics are linked to higher risk. - Achieving an ideal occlusion does not prevent TMD, and no method of prevention has been proven effective. TMD is usually alleviated by simple, conservative treatments in most cases.

































































