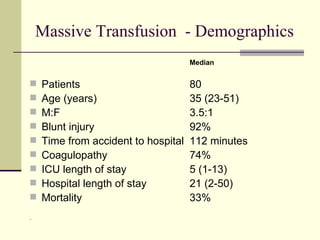
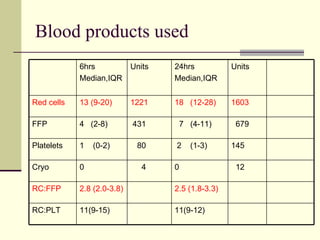
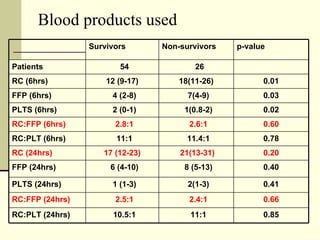
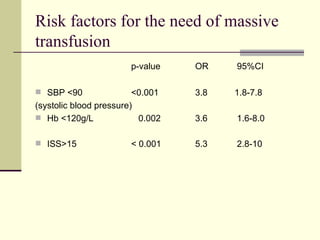
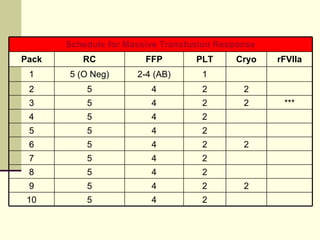
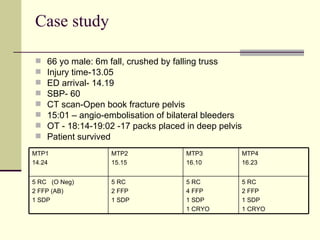
Massive transfusion protocols aim to replace lost blood volume and prevent coagulopathy in severely injured trauma patients. The study found that 7% of trauma patients received over 10 units of red blood cells in the first 24 hours, identifying them at high risk. Early administration of blood products in a 1:1:1 ratio of red cells, plasma, and platelets according to massive transfusion protocols was associated with reduced mortality compared to standard transfusion practices. Simple clinical factors like low blood pressure, high injury severity score, and coagulopathy can help predict patients needing massive transfusion.


![Results TOTAL 6488 trauma patients 438 (7%) received transfusion 358 received 1-9 red cells and 80 received ≥10 red cells. Major trauma (ISS>15) - 1021 patients 313 (30%) were transfused ISS [16-24] - 19% ISS [25-49] - 45% ISS [50-75] - 8%](https://image.slidesharecdn.com/massivetransfusionintrauma-122613320433-phpapp03/85/Massive-Transfusion-In-Trauma-6-320.jpg)