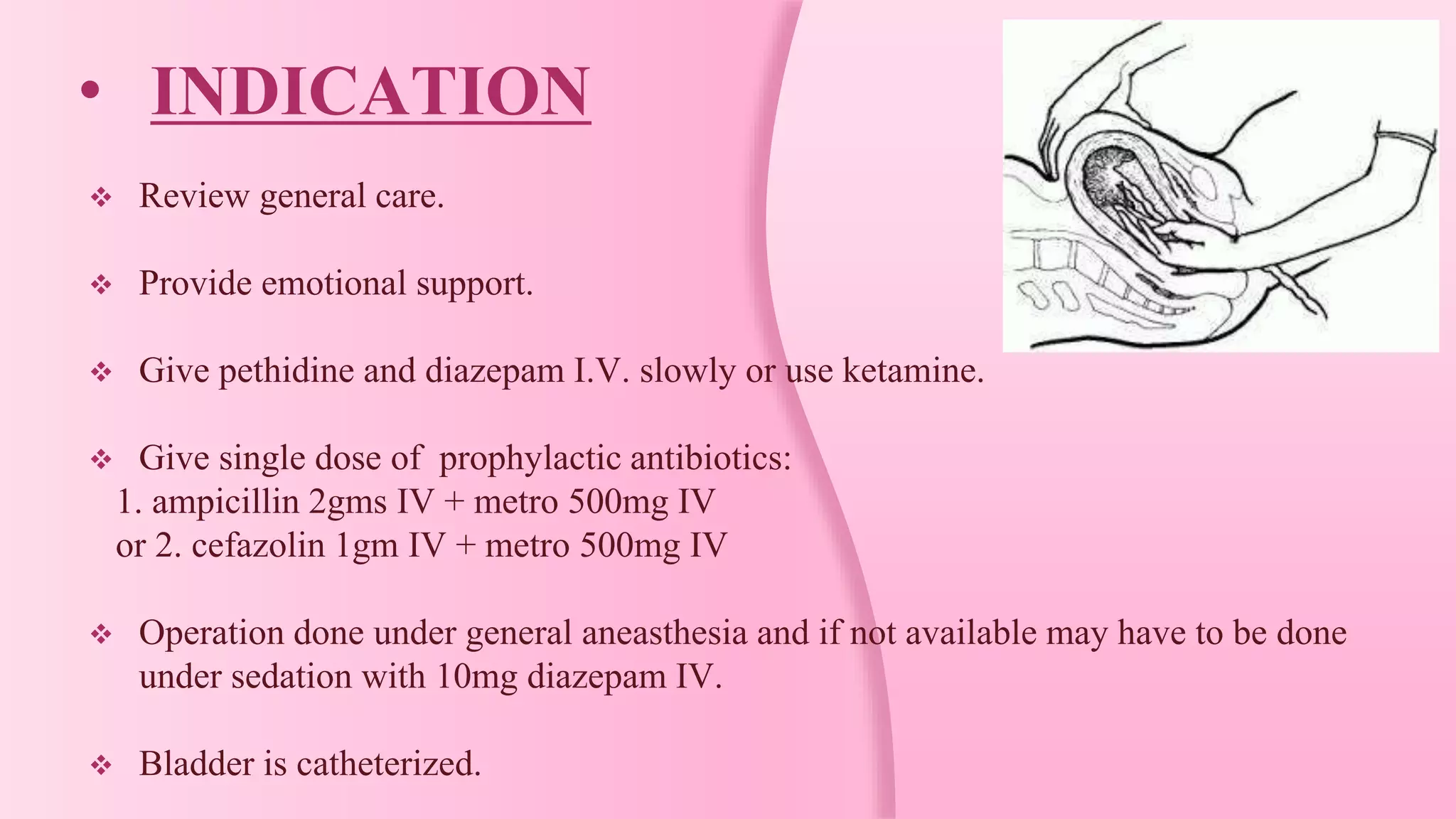
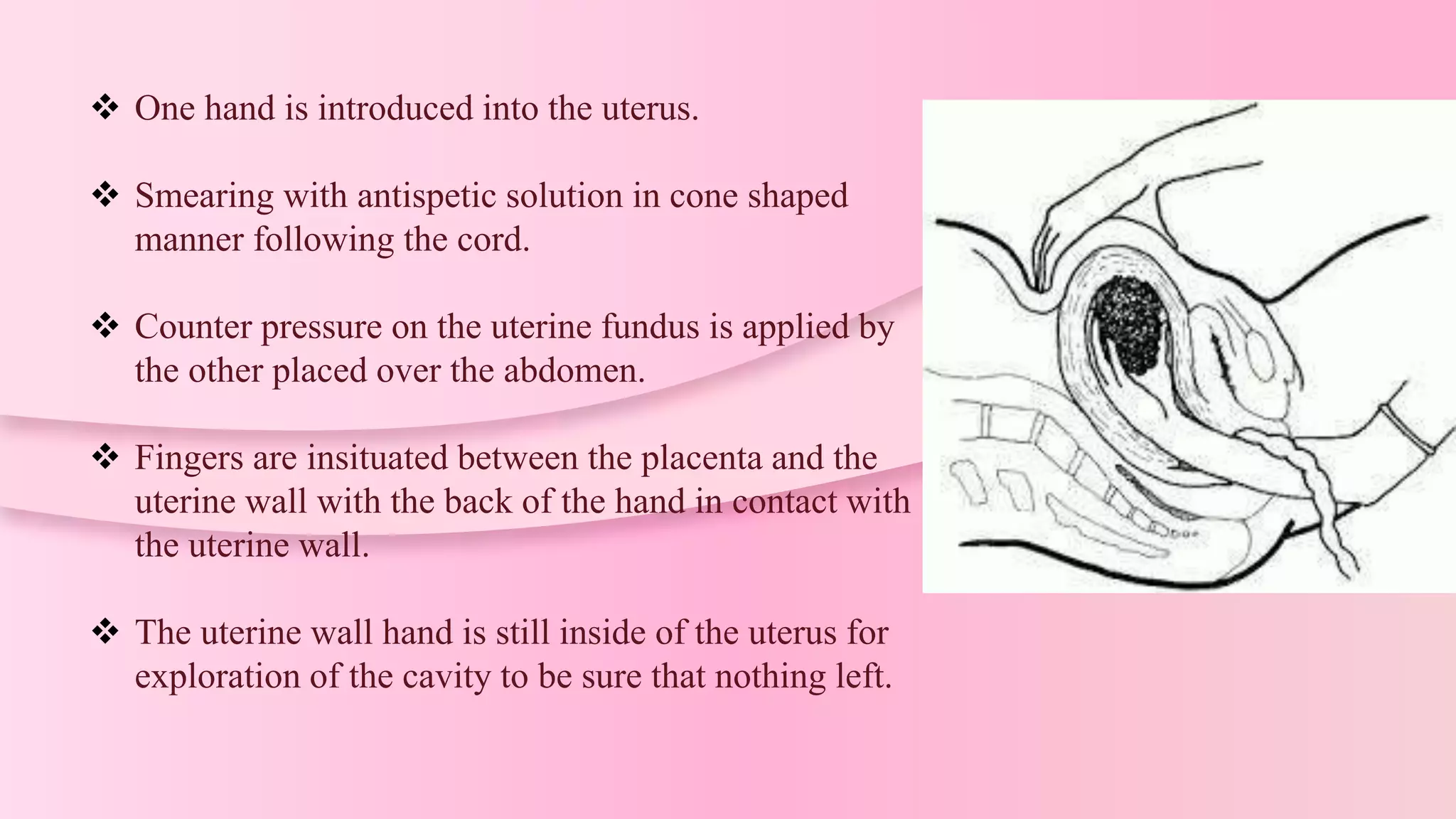
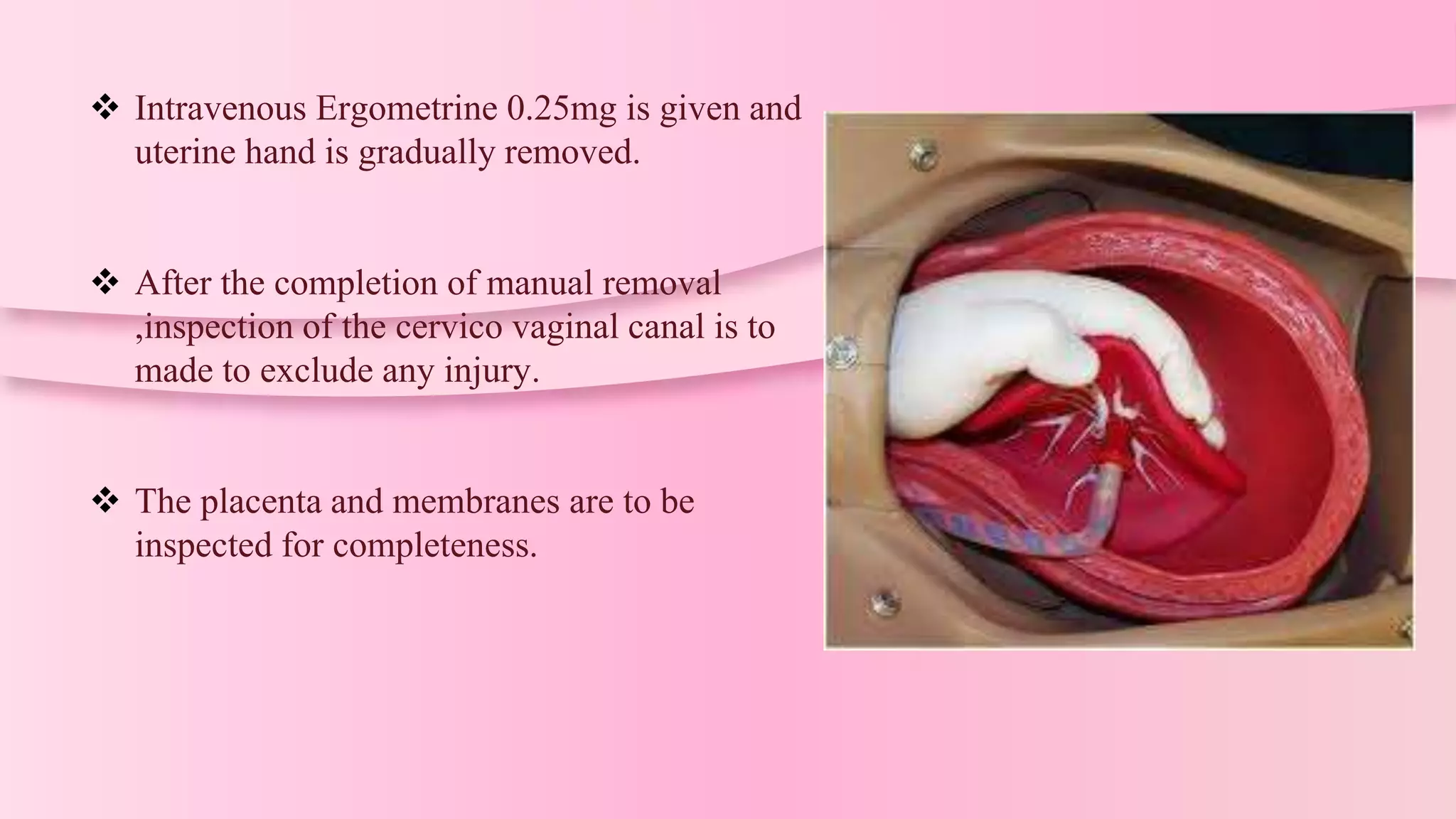
Manual removal of placenta (MRP) is a procedure to remove a retained placenta from the uterus after childbirth. It is performed under general anesthesia or deep sedation with the patient in lithotomy position after catheterizing the bladder. One hand is inserted into the uterus to locate the placenta and separate it from the uterine wall with a sawing motion while applying counter pressure on the abdomen. The placenta is then extracted while massaging the uterus, and ergometrine is injected to ensure uterine contraction. Complications can include hemorrhage, injury, infection or inversion if not performed correctly.