Downloaded 68 times


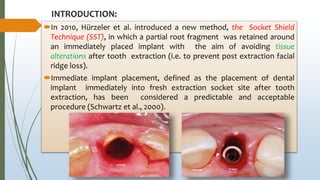
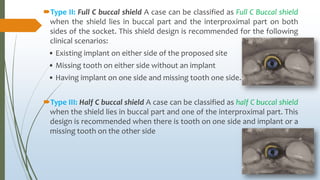
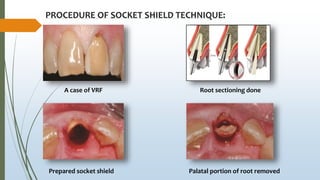
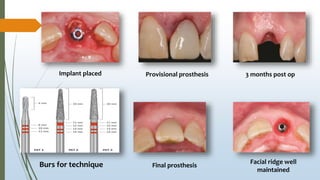



The document discusses the socket-shield technique, introduced in 2010 to help preserve buccal tissues during immediate implant placements by retaining a portion of the root post-extraction. It outlines indications, contraindications, procedural steps, advantages, limitations, and complications associated with the technique, emphasizing its potential benefits for maintaining ridge contour and minimizing surgery-associated tissue loss. The summary concludes with a mention of the technique's rising popularity and relevance in preserving hard and soft tissues post-tooth extraction.





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















