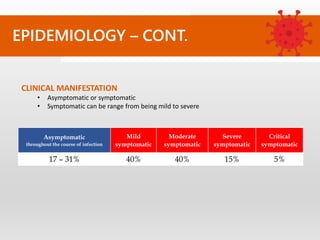
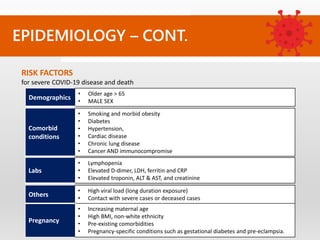
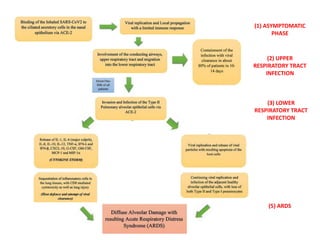
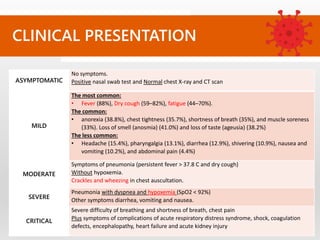
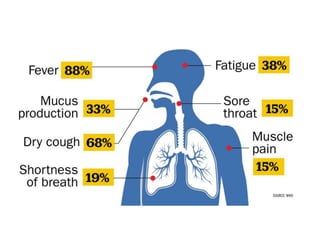
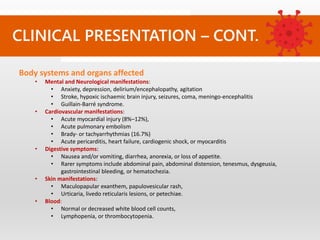
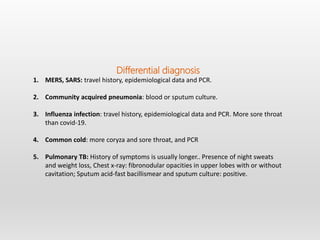
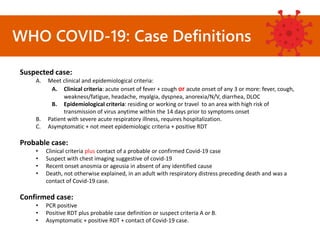
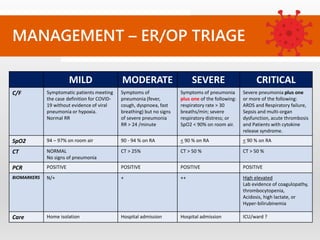
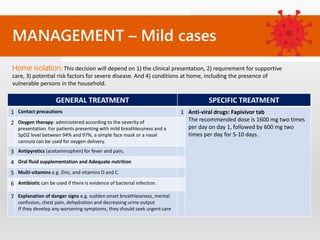
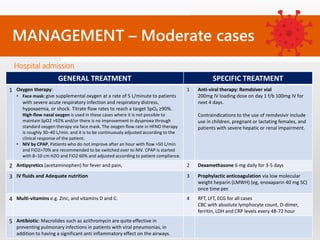
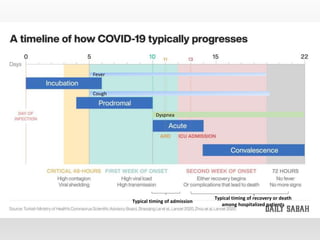
The document details COVID-19, an infectious disease caused by SARS-CoV-2, outlining its transmission, clinical manifestations, risk factors, and management strategies. It discusses the virus's pathophysiology, including asymptomatic and symptomatic phases, and provides diagnostic criteria along with laboratory tests for identification and severity assessment. Management protocols for mild, moderate, severe, and critical cases are also elaborated, emphasizing the importance of antiviral therapy, oxygen support, and monitoring of comorbidities.