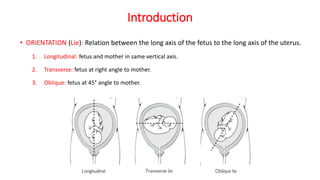
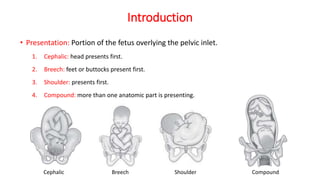
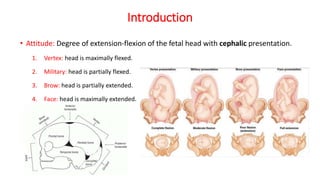
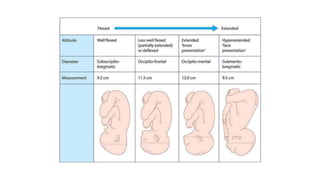
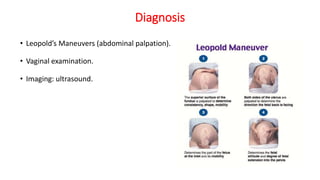
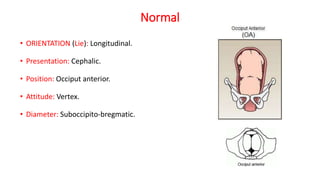
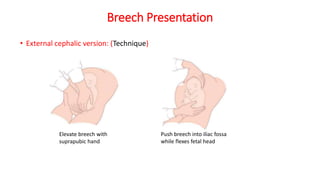
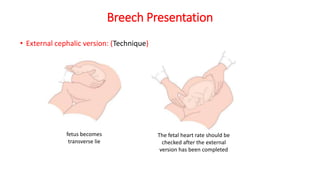
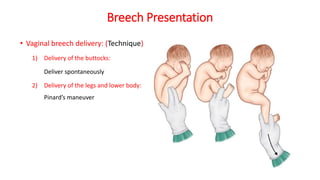
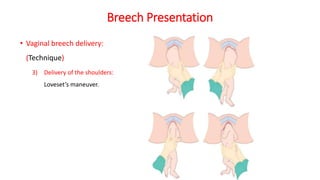
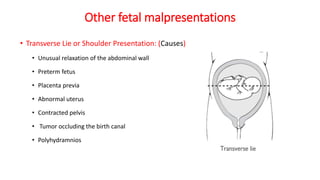
This document outlines various fetal malpresentations and malpositions that can occur during labor and delivery. It discusses normal presentation and position, as well as abnormal presentations including occiput posterior, face, brow, breech, transverse lie, shoulder, and compound. For each presentation, the document describes causes, diagnosis techniques including Leopold's maneuvers and ultrasound, and approaches to delivery management. Breech presentation is discussed in particularly depth, outlining types of breech, risk factors, techniques for external cephalic version and vaginal breech delivery.














































































![제 23회 보아즈(BOAZ) 빅데이터 컨퍼런스 - [MBOAX] : ABSA를 활용한 소비자 반응 분석 기반 운영 효율화 대시보드 설계](https://cdn.slidesharecdn.com/ss_thumbnails/3-1boaz23rdconferencemboax-260203102709-9d519923-thumbnail.jpg?width=640&height=640&fit=bounds)




