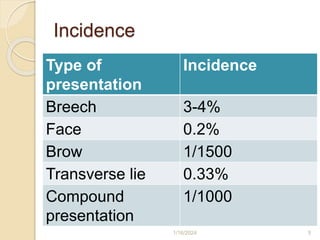
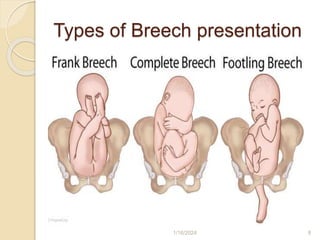
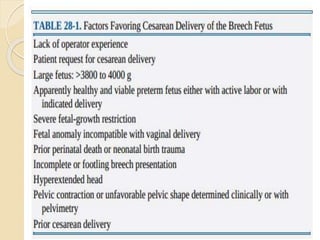
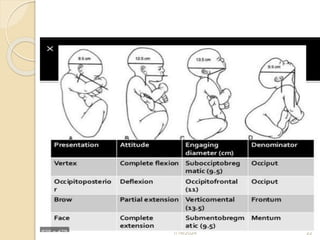
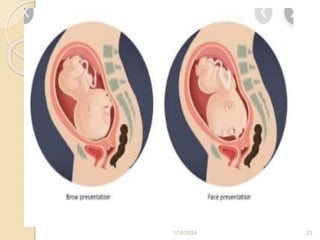
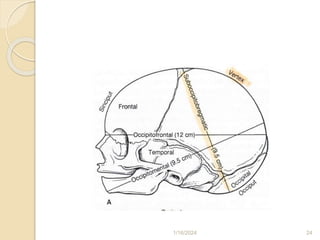
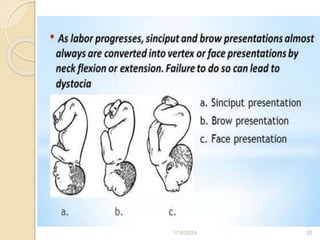
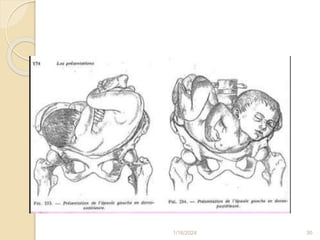
This document defines malpresentations as any fetal position other than vertex presentation. It discusses the most common types including breech, brow, shoulder, face, compound, and parietal bone presentations. Causes of malpresentations include prematurity, high parity, fetal anomalies, and others. Incidence rates are provided for different presentation types. The document then goes into further detail about breech, face, brow, transverse lie, and compound presentations, defining each type, discussing causes, diagnosis, management considerations, and risks. Management may include external cephalic version, cesarean delivery, or attempted vaginal breech delivery depending on the situation.