Downloaded 30 times

![Physician Payment
3
Based on a complicated formula:
– Facility or Non-Facility Pricing Amount =
[(Work RVU * Work GPCI) +
(Transitioned Facility or Non-Facility PE RVU * PE GPCI) +
(MP RVU * MP GPCI)] * Conversion Factor (CF)
Initial conversion factor was created in 1992 and
adjusted annually based on three factors:
– The Medicare Economic Index (MEI)
– RVU budget neutrality
– Medicare expenditures for physician services as
compared to a sustainable growth rate](https://image.slidesharecdn.com/macraproposedruleissuesopportunities-160601152227/75/MACRA-Proposed-Rule-Issues-Opportunities-3-2048.jpg)






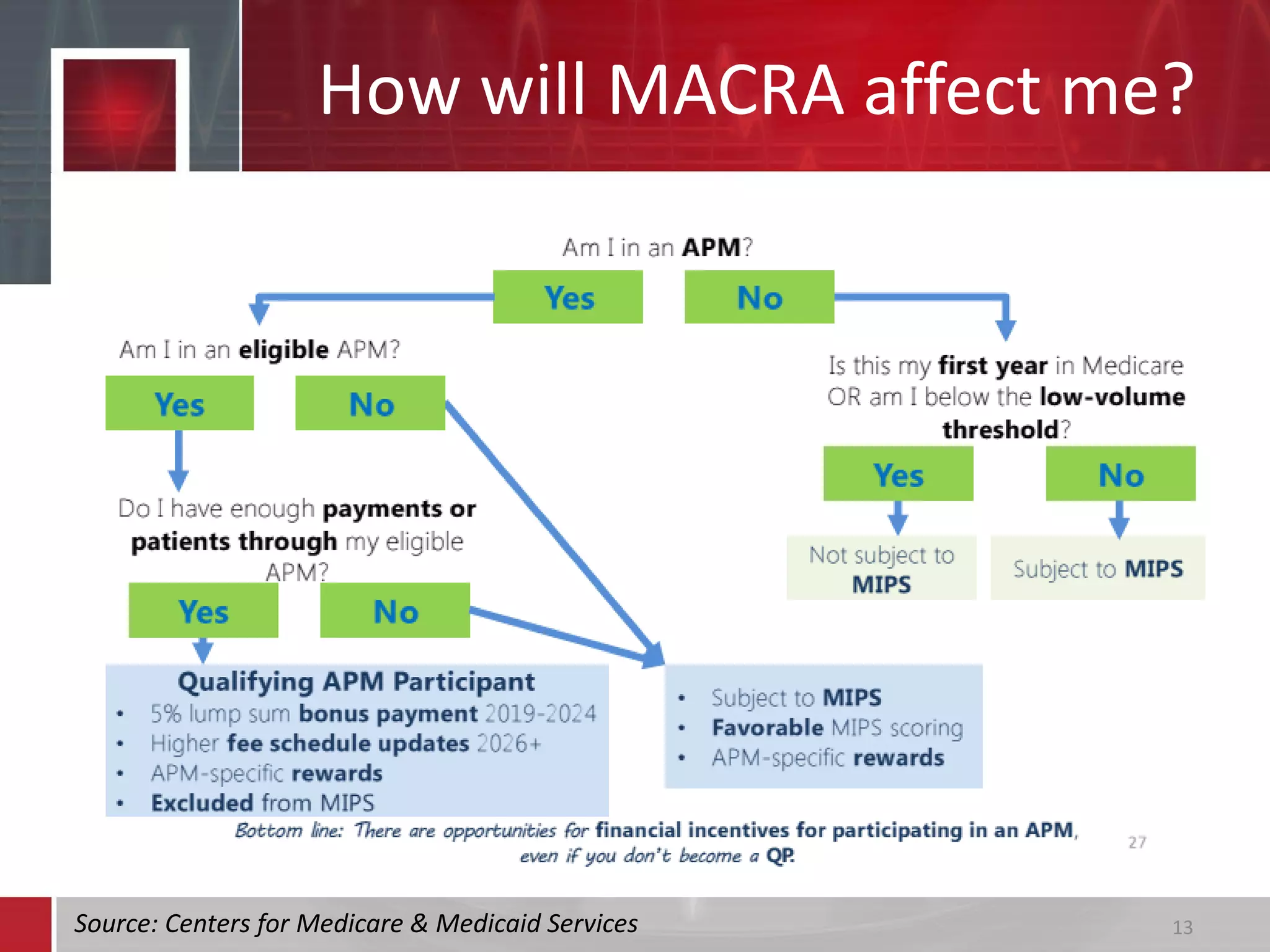
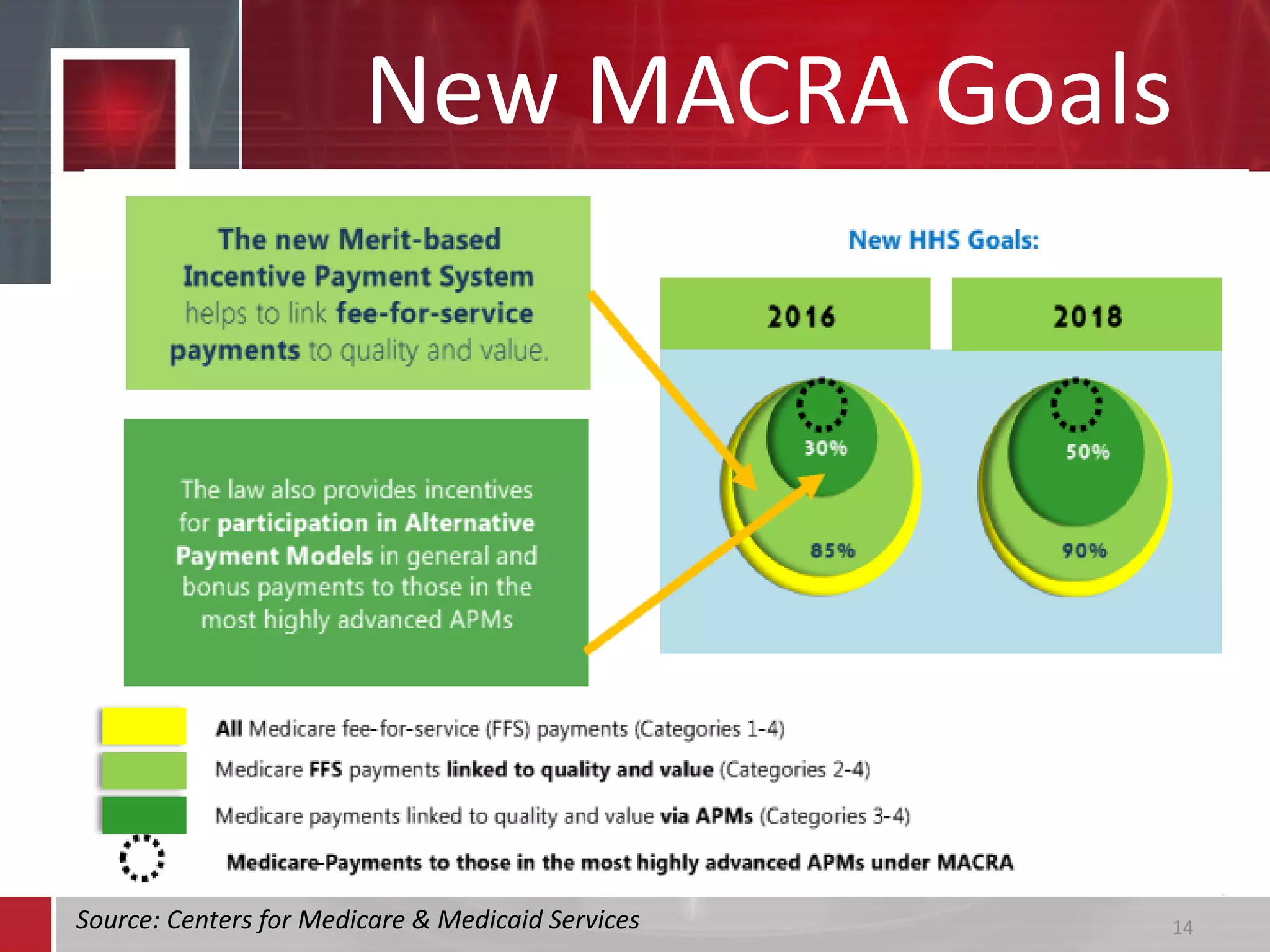



























The document discusses the Medicare Access and CHIP Reauthorization Act (MACRA), outlining its introduction, major changes such as the repeal of the Sustainable Growth Rate (SGR), and the establishment of the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs). It details how MIPS adjusts Medicare reimbursement based on performance scores in quality, resource use, and clinical practice improvement while offering different options for physicians to participate in either MIPS or APMs. Additionally, it highlights the implications of these new systems on physician payment frameworks and the shift towards incentivizing quality and value in healthcare delivery.






































































































