Download as PDF, PPTX
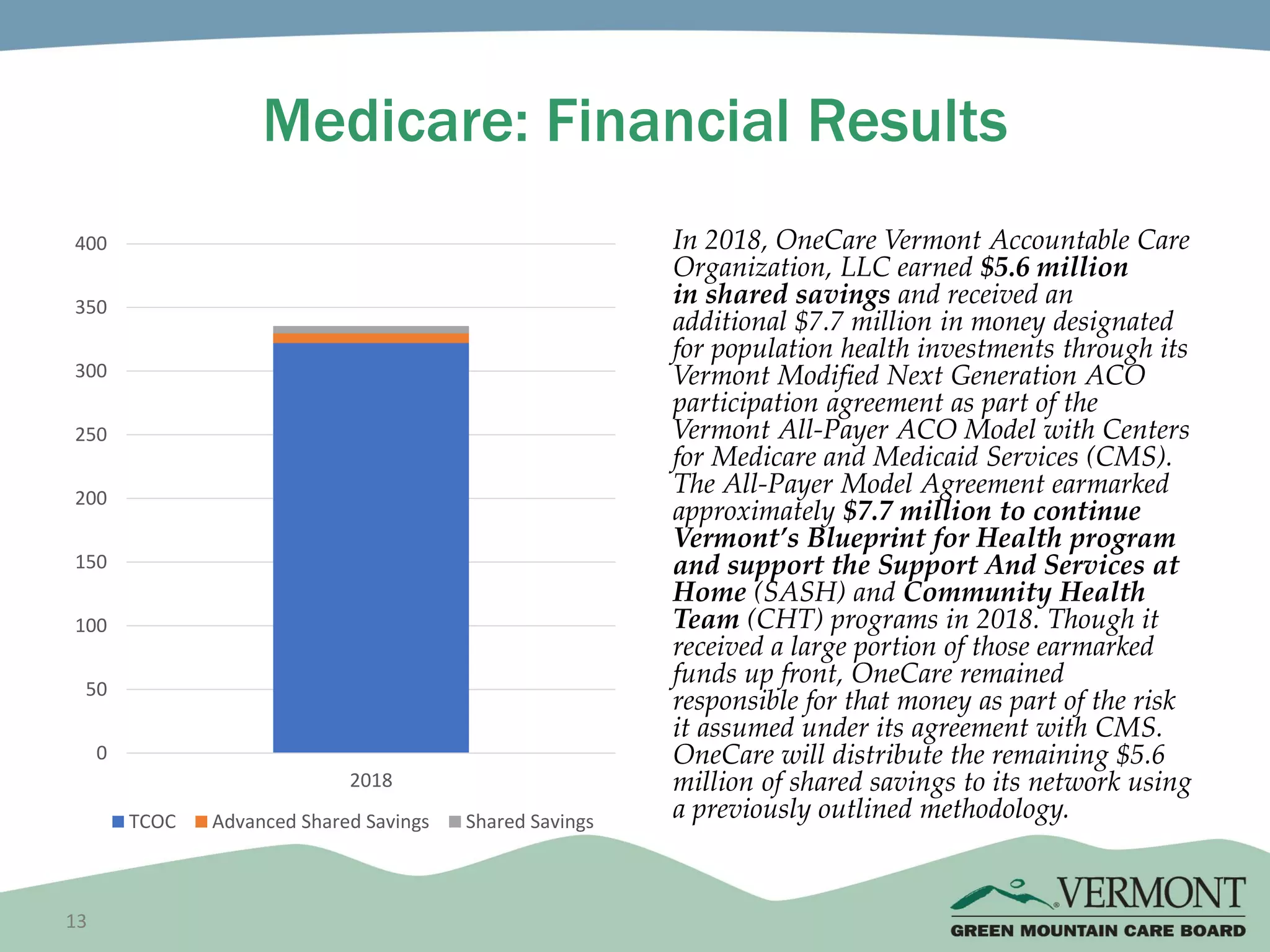
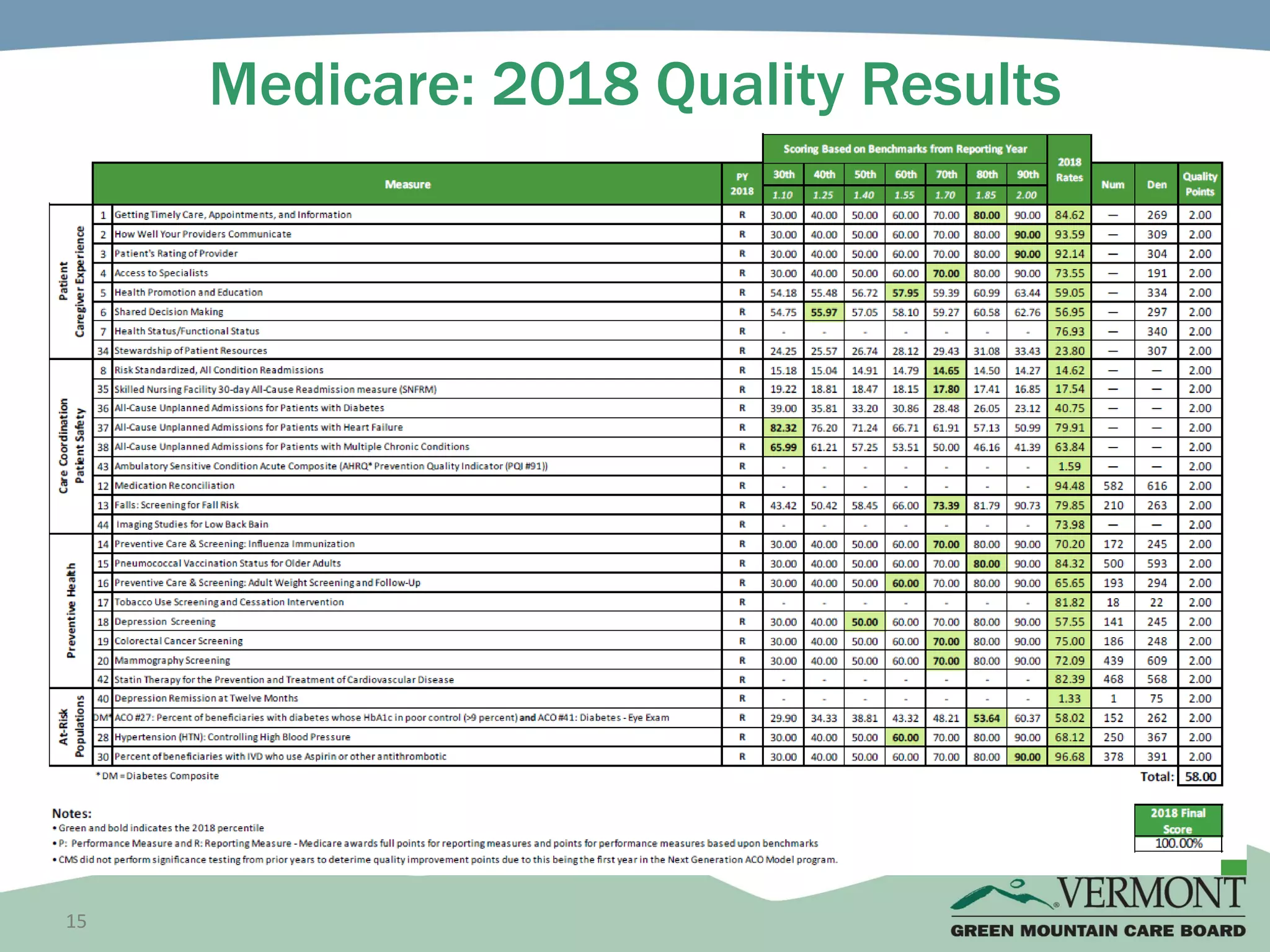
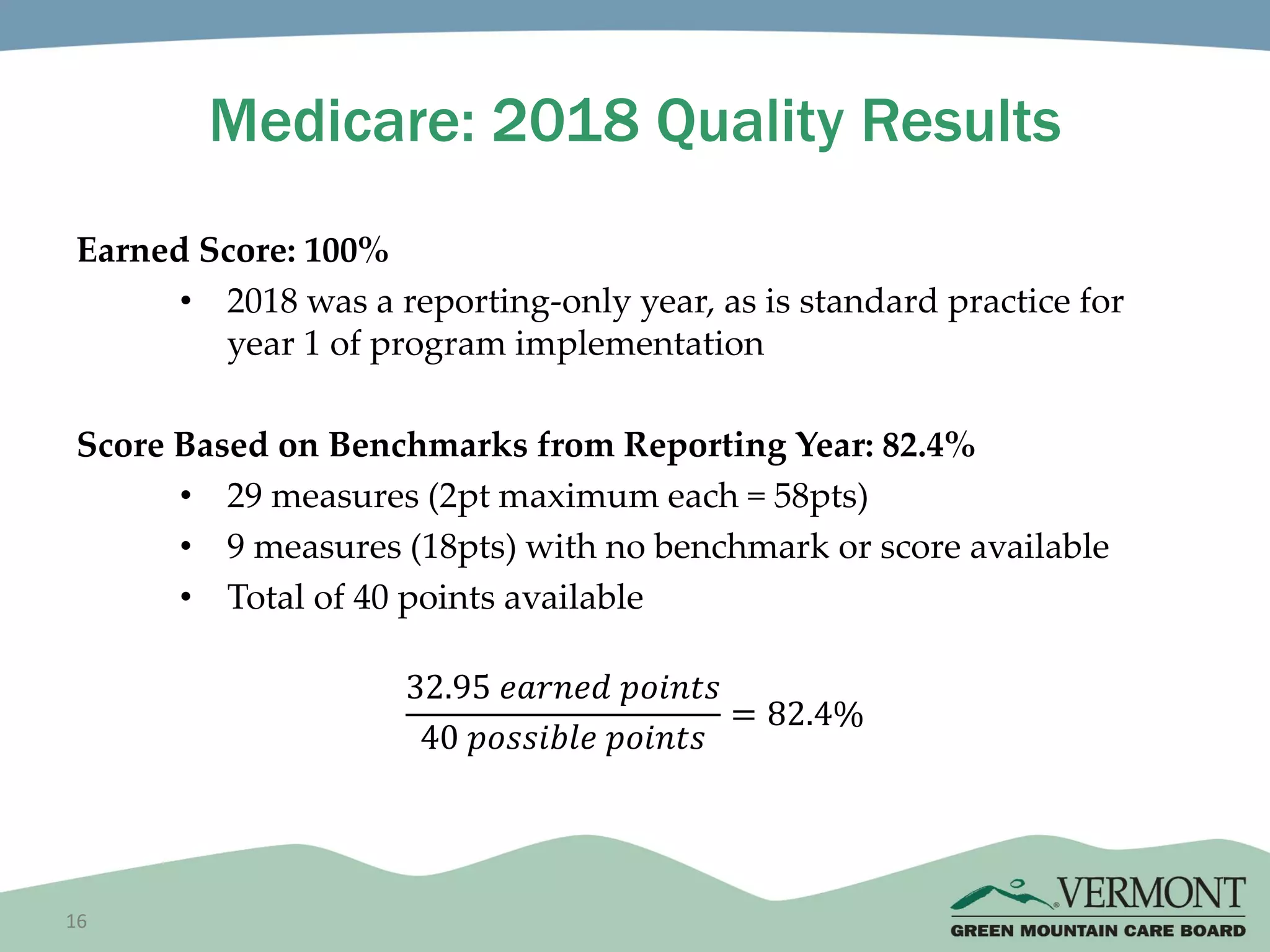
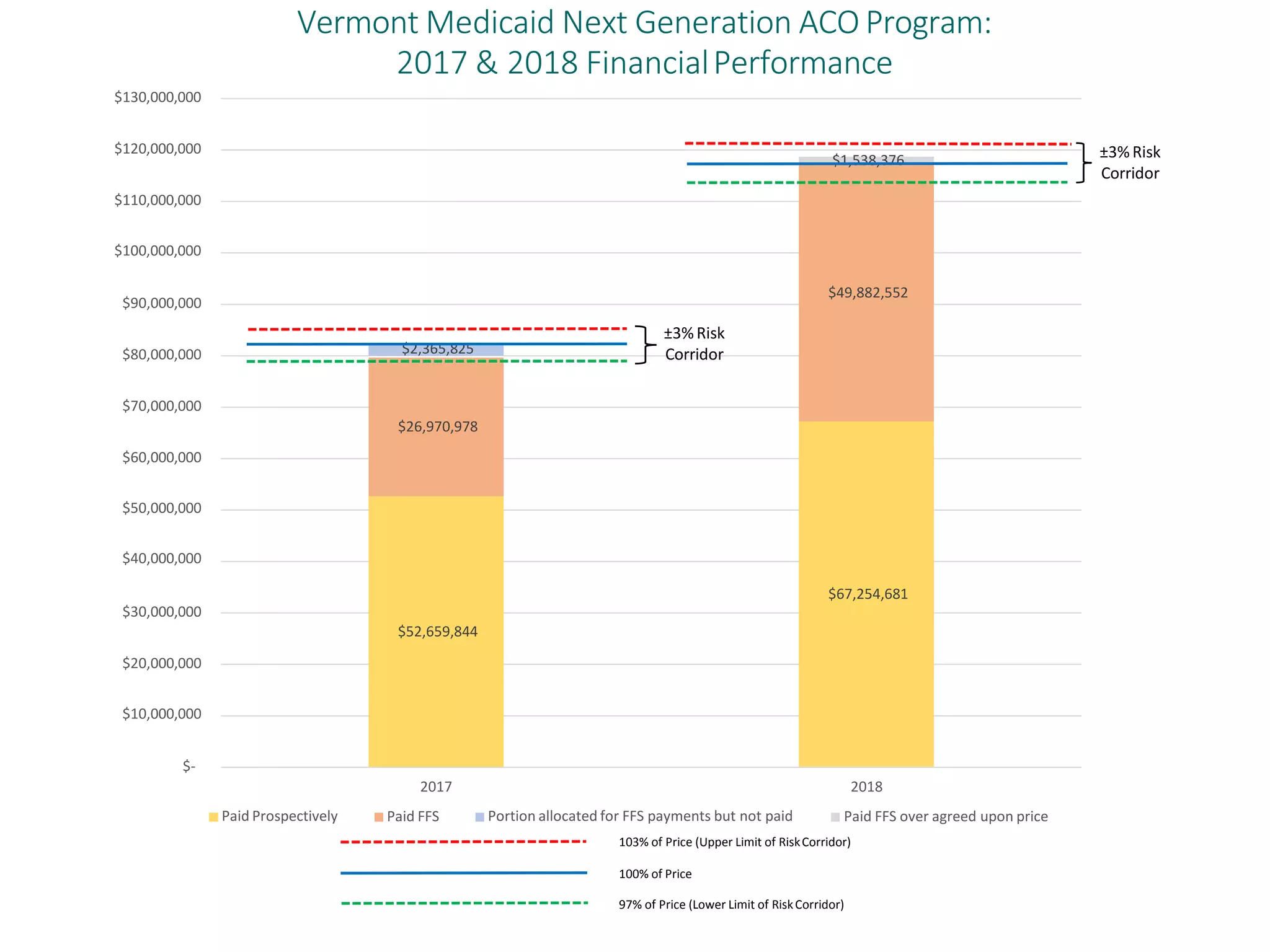
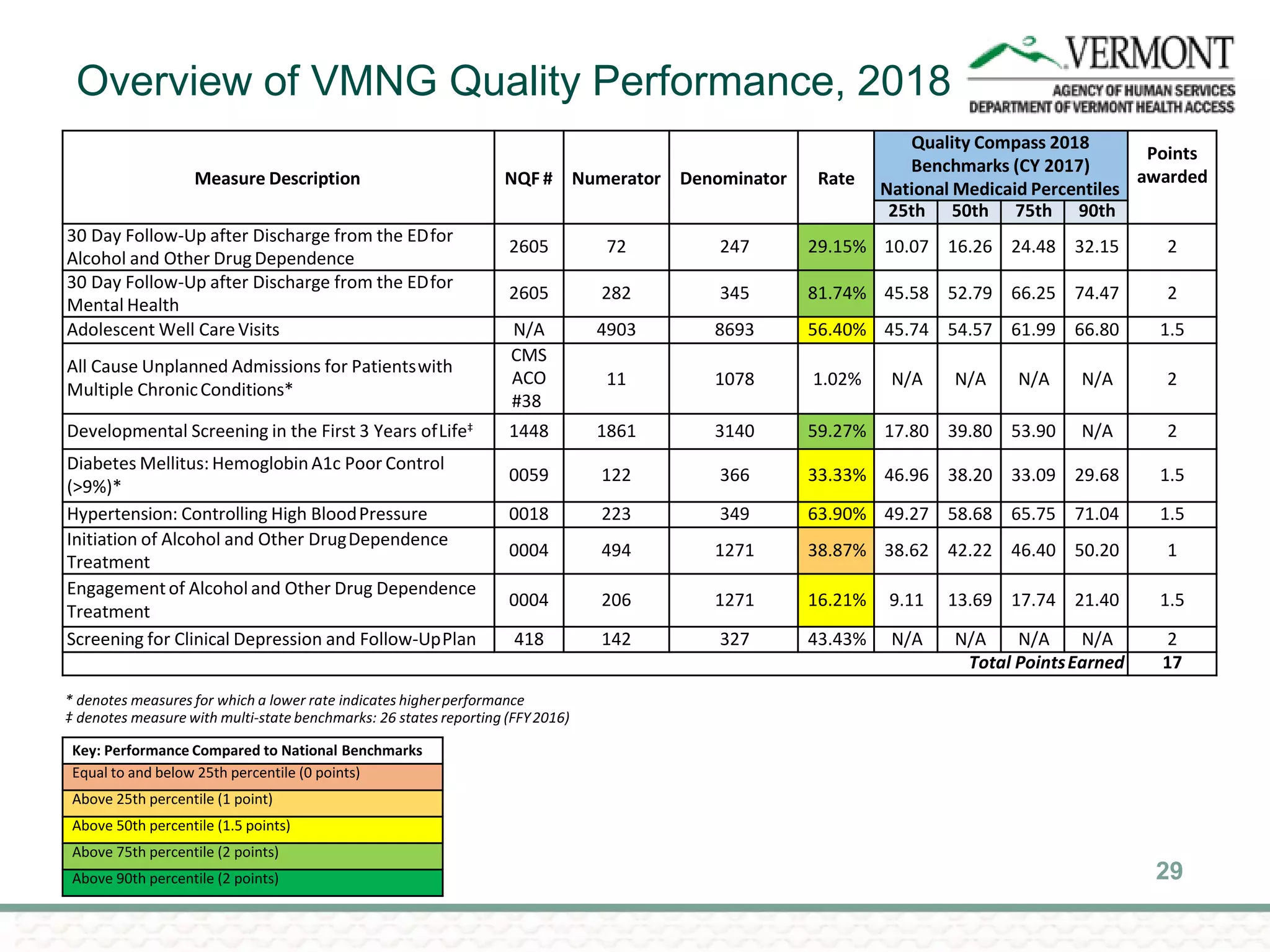

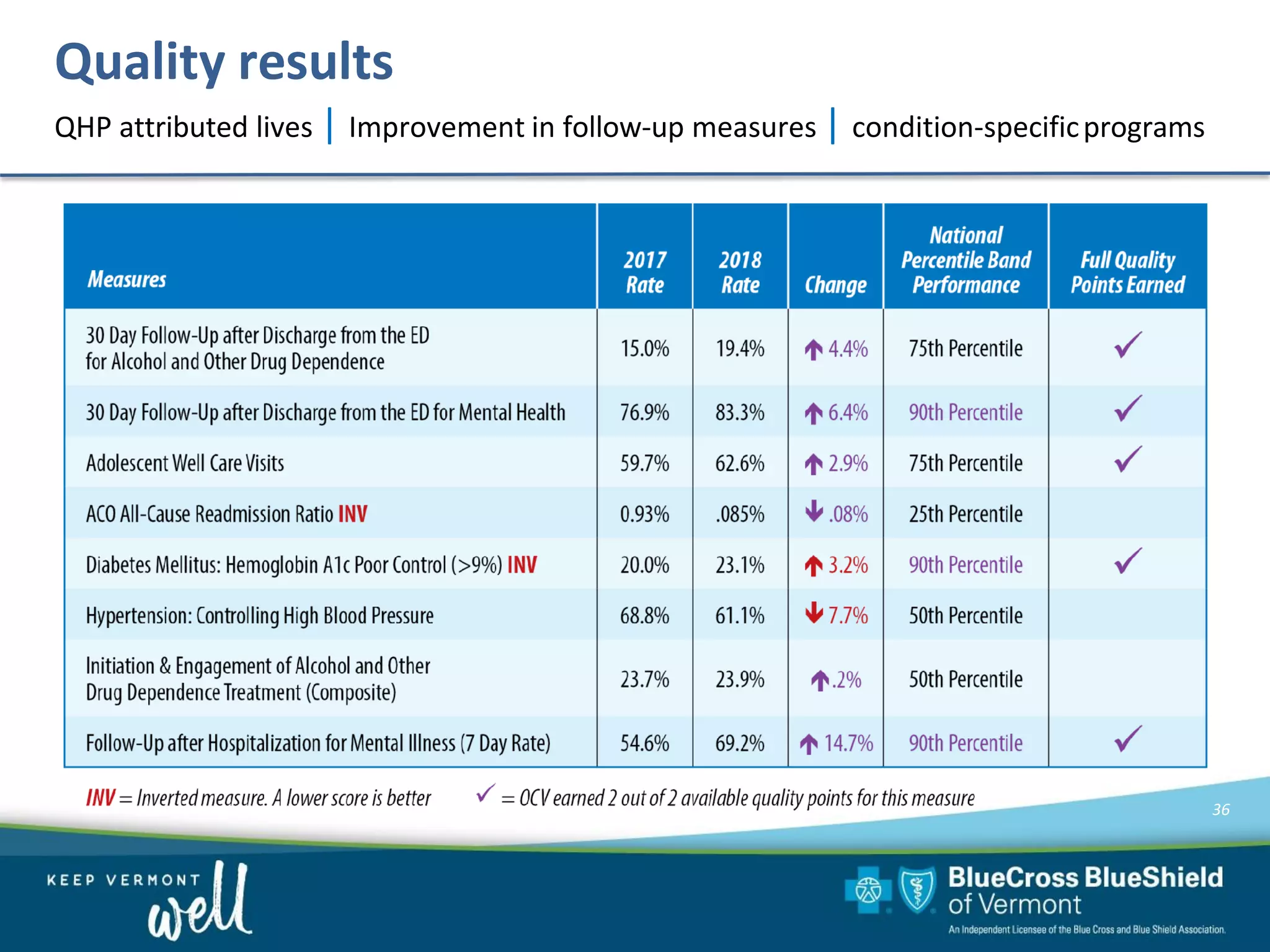

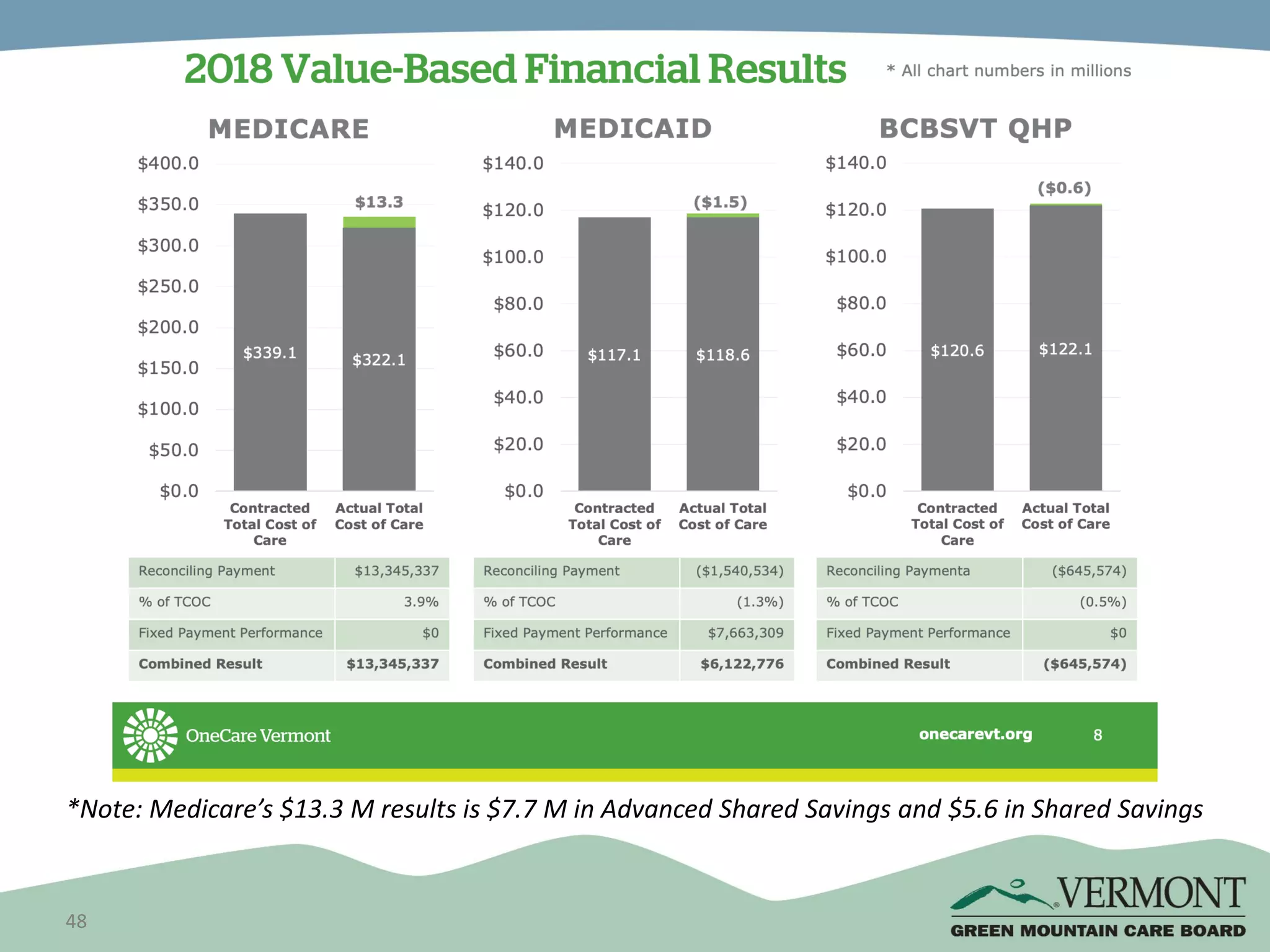

OneCare Vermont's ACO providers met most quality targets and earned $5.6 million in shared savings from Medicare in 2018. The ACO scored 100% on Medicare quality measures in the reporting year, earning 82.4% of available points compared to benchmarks. For Medicaid, the ACO was within the ±3% risk corridor, providing $1.5 million more in care than expected. The ACO met quality targets on 85% of measures, exceeding national benchmarks for developmental screening and follow-up after emergency department visits.























































































