Downloaded 20 times

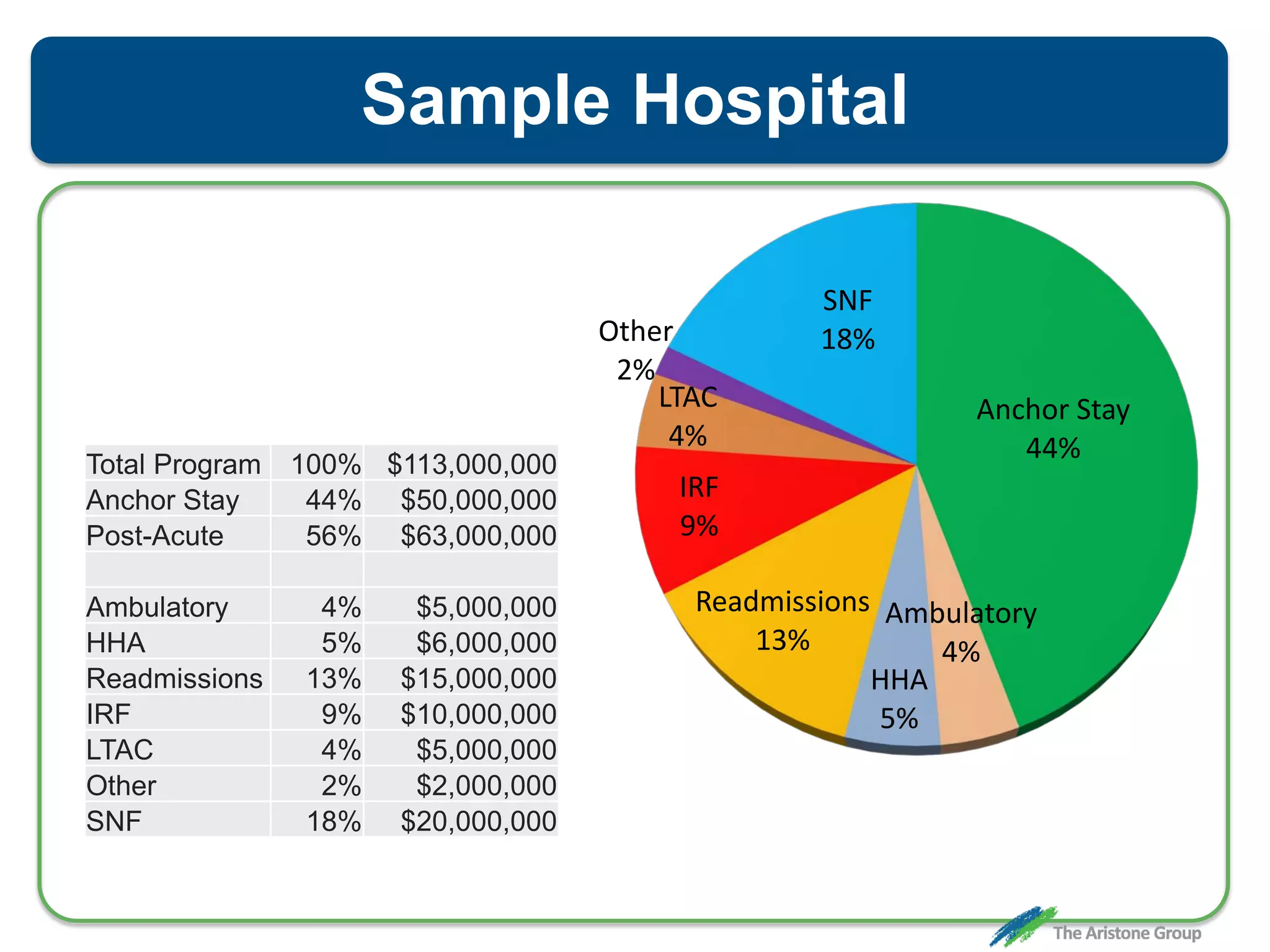
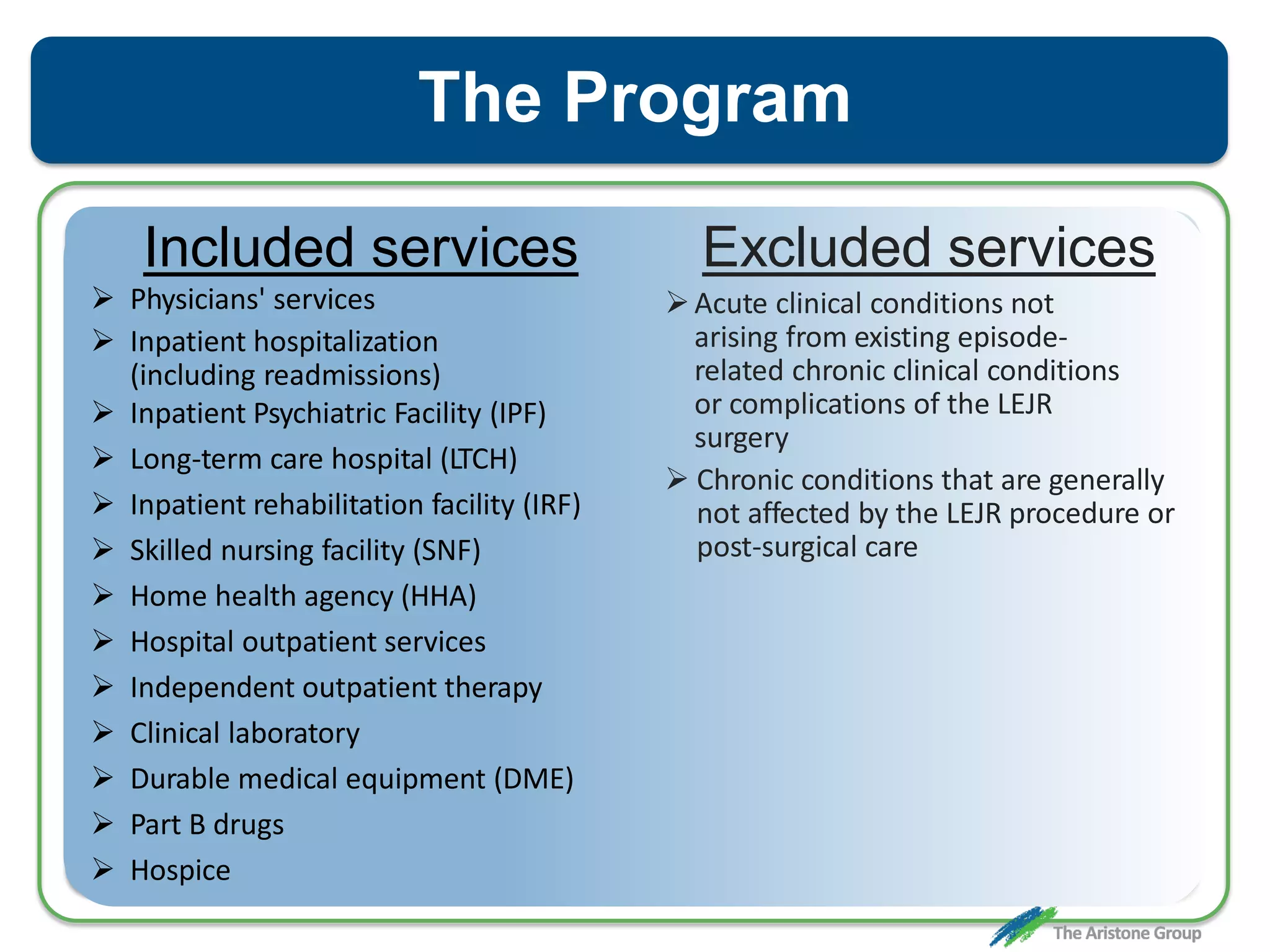
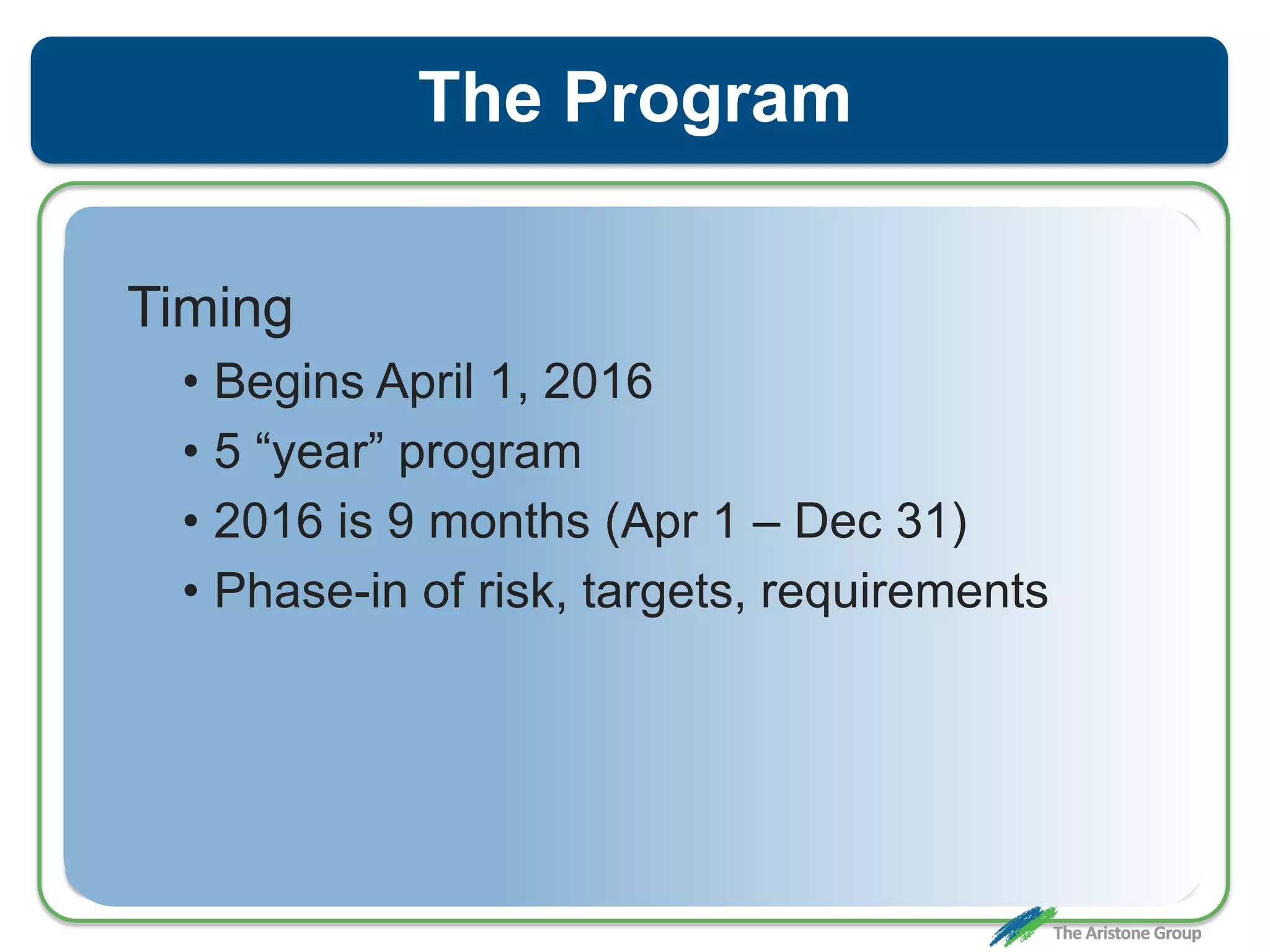
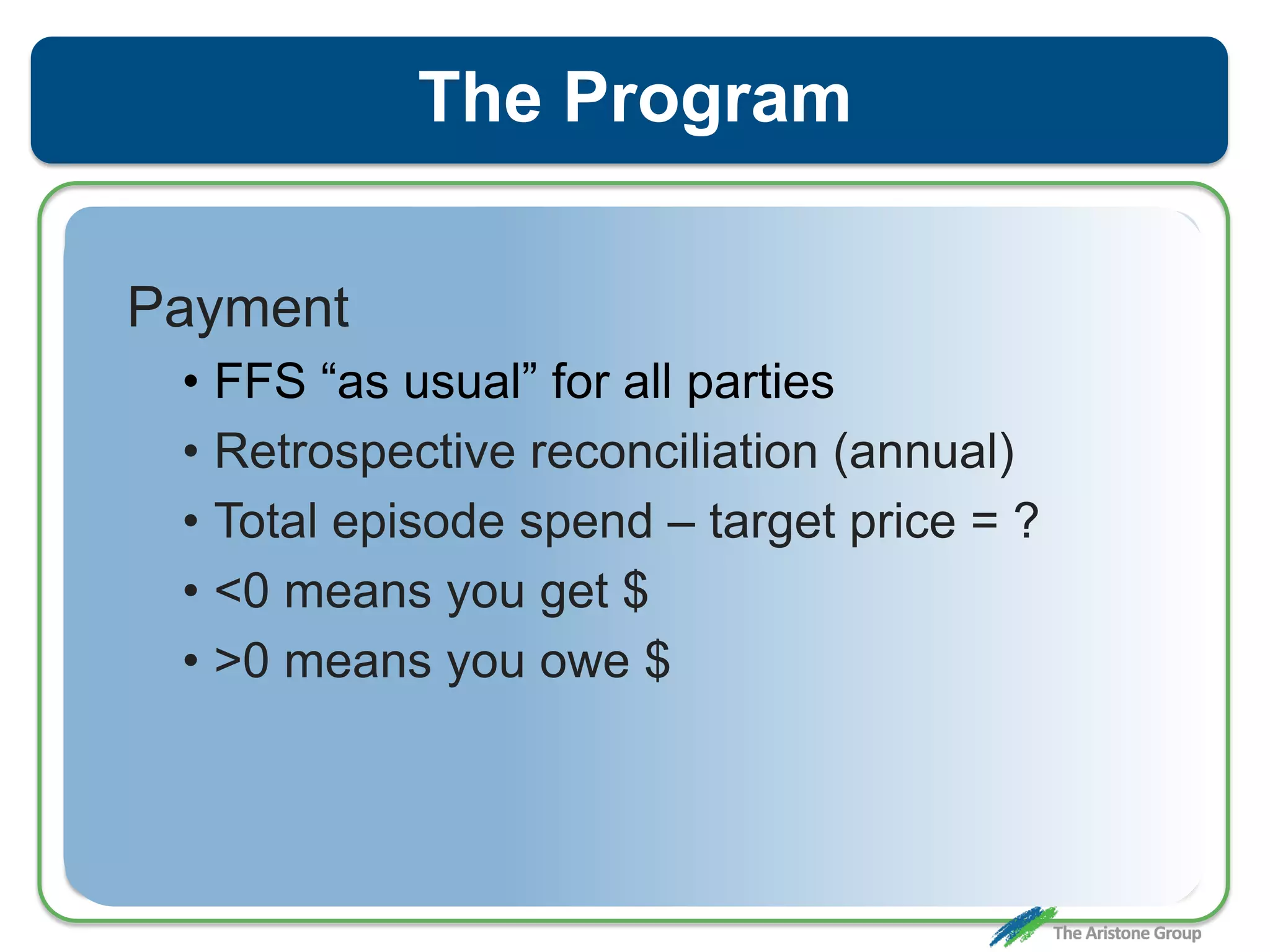
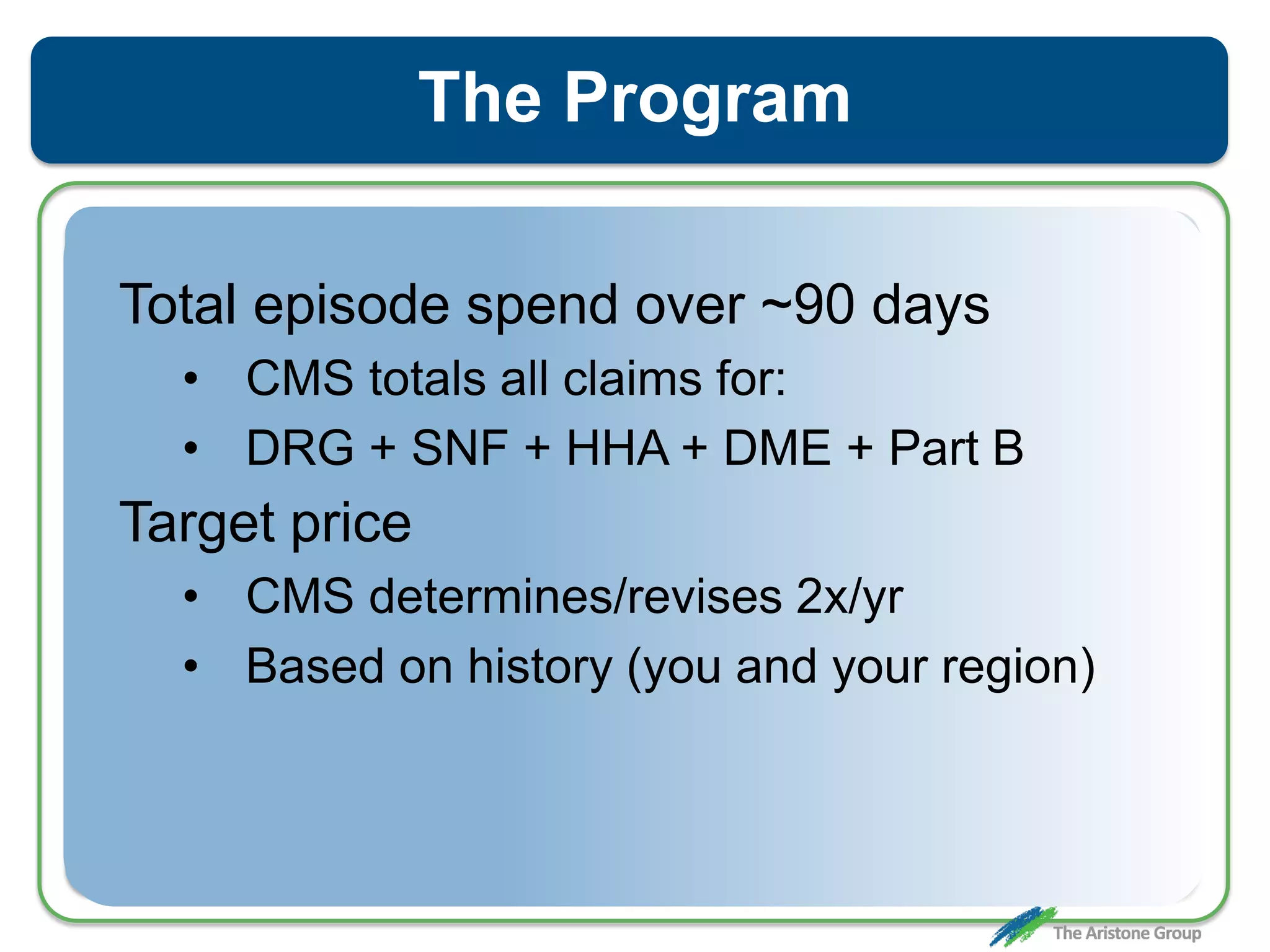
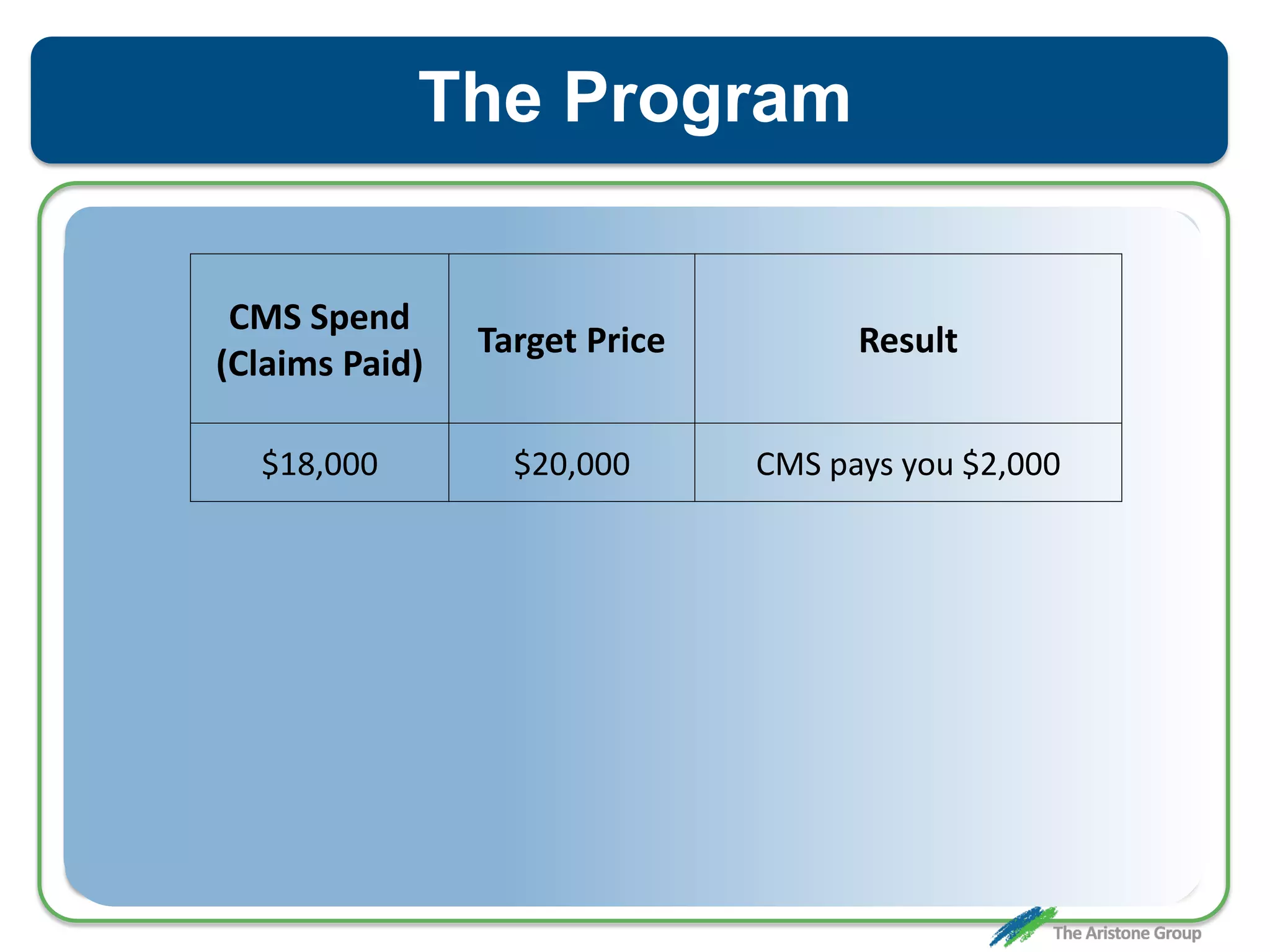
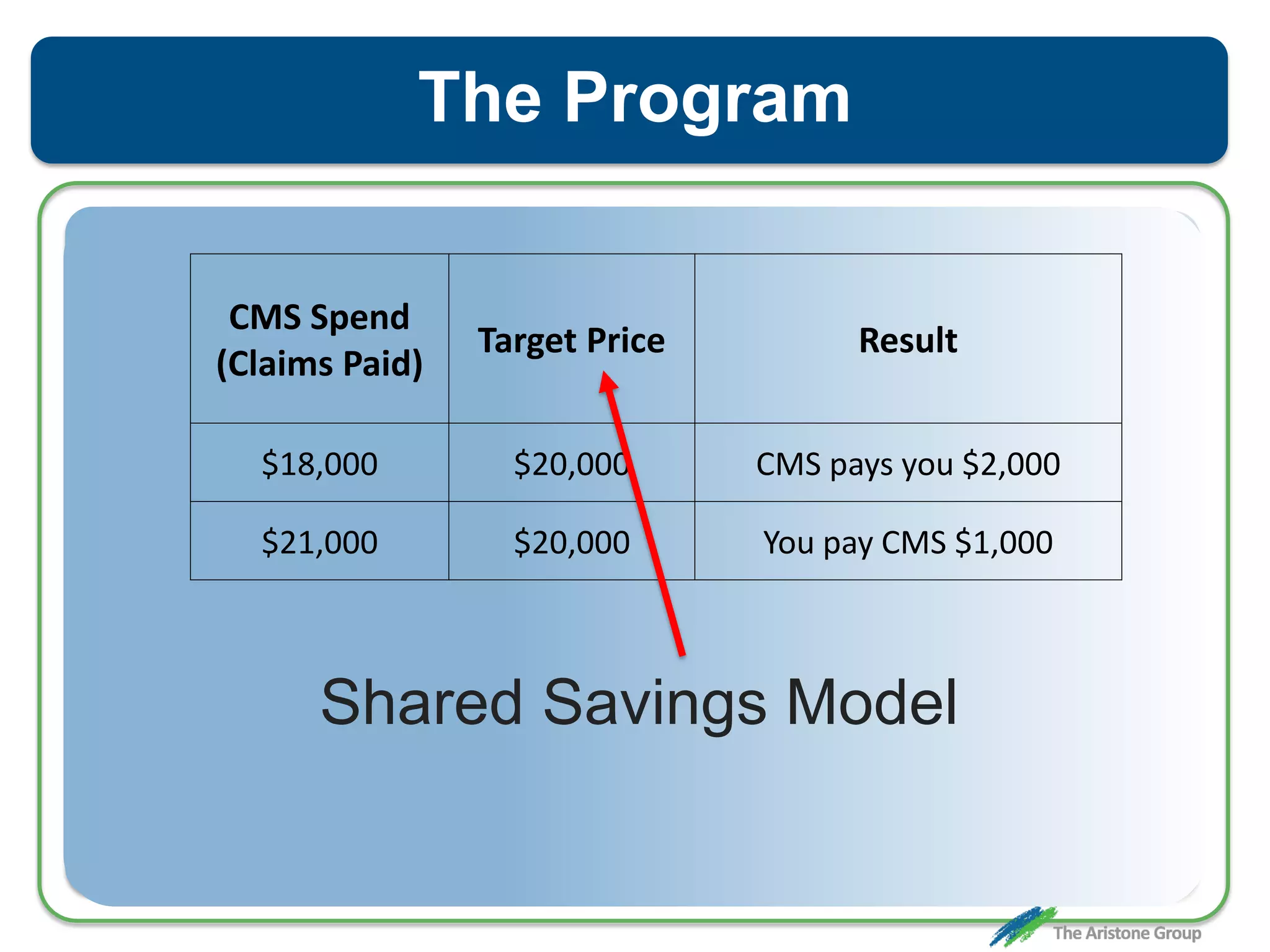
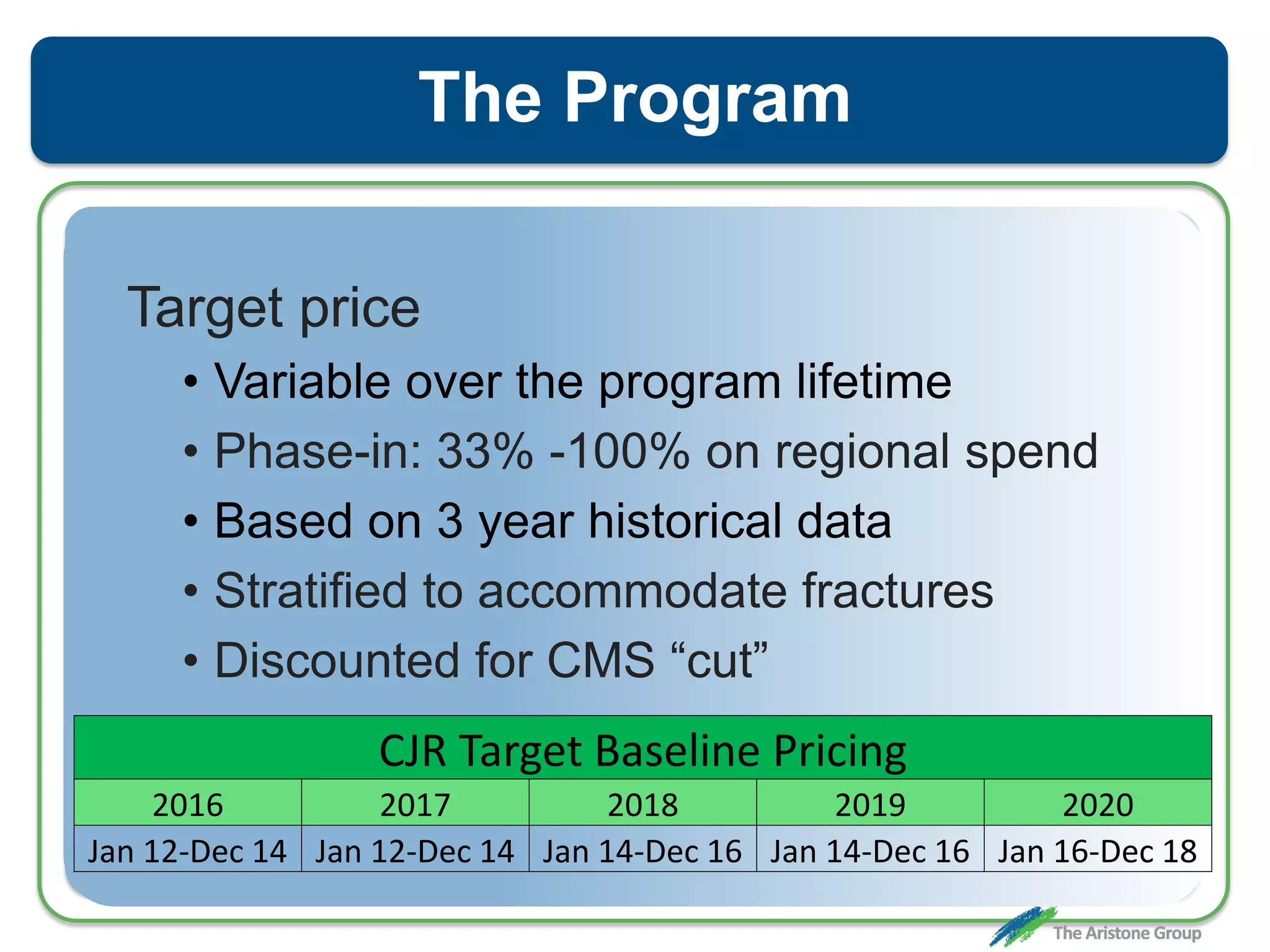
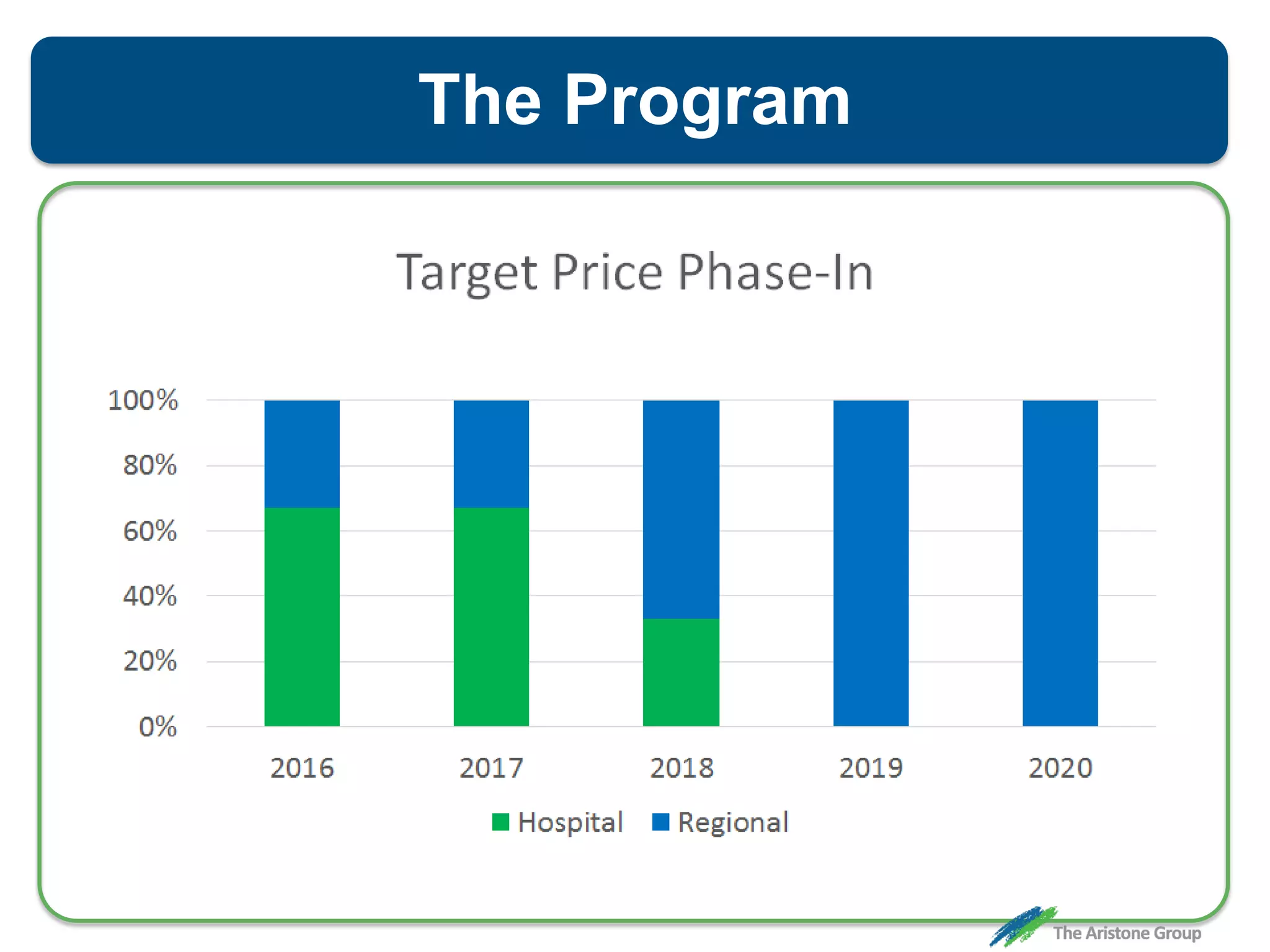
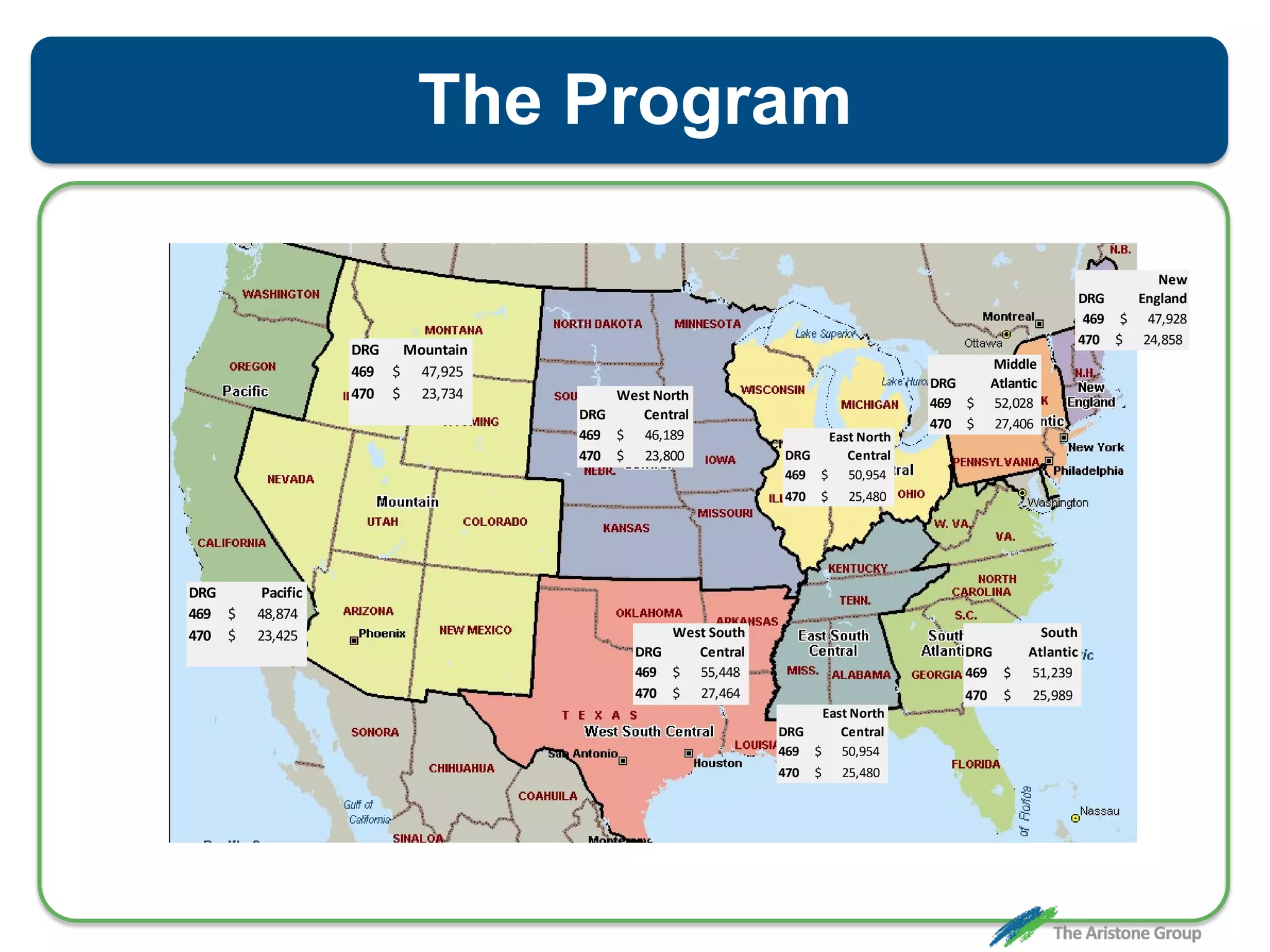
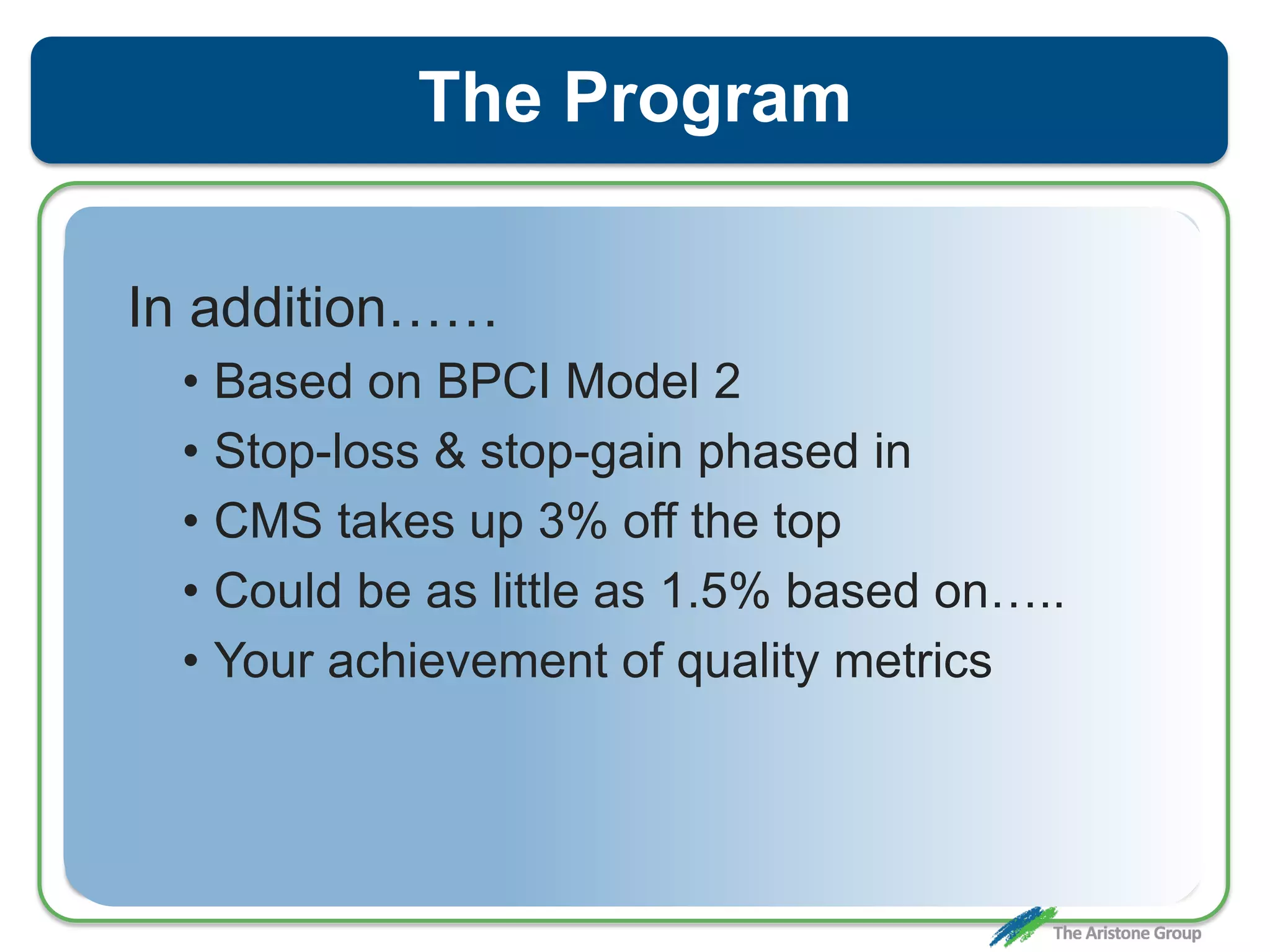
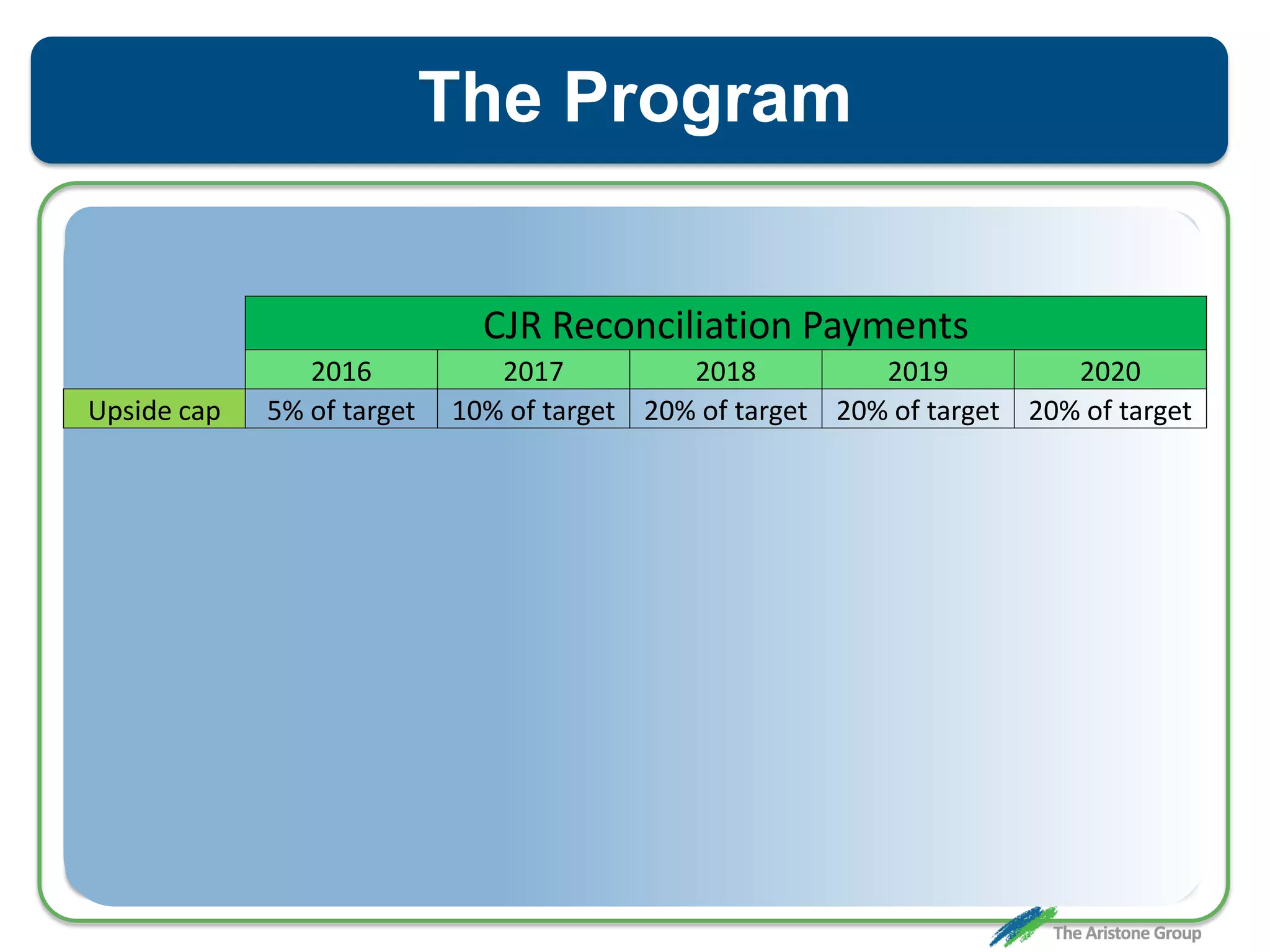
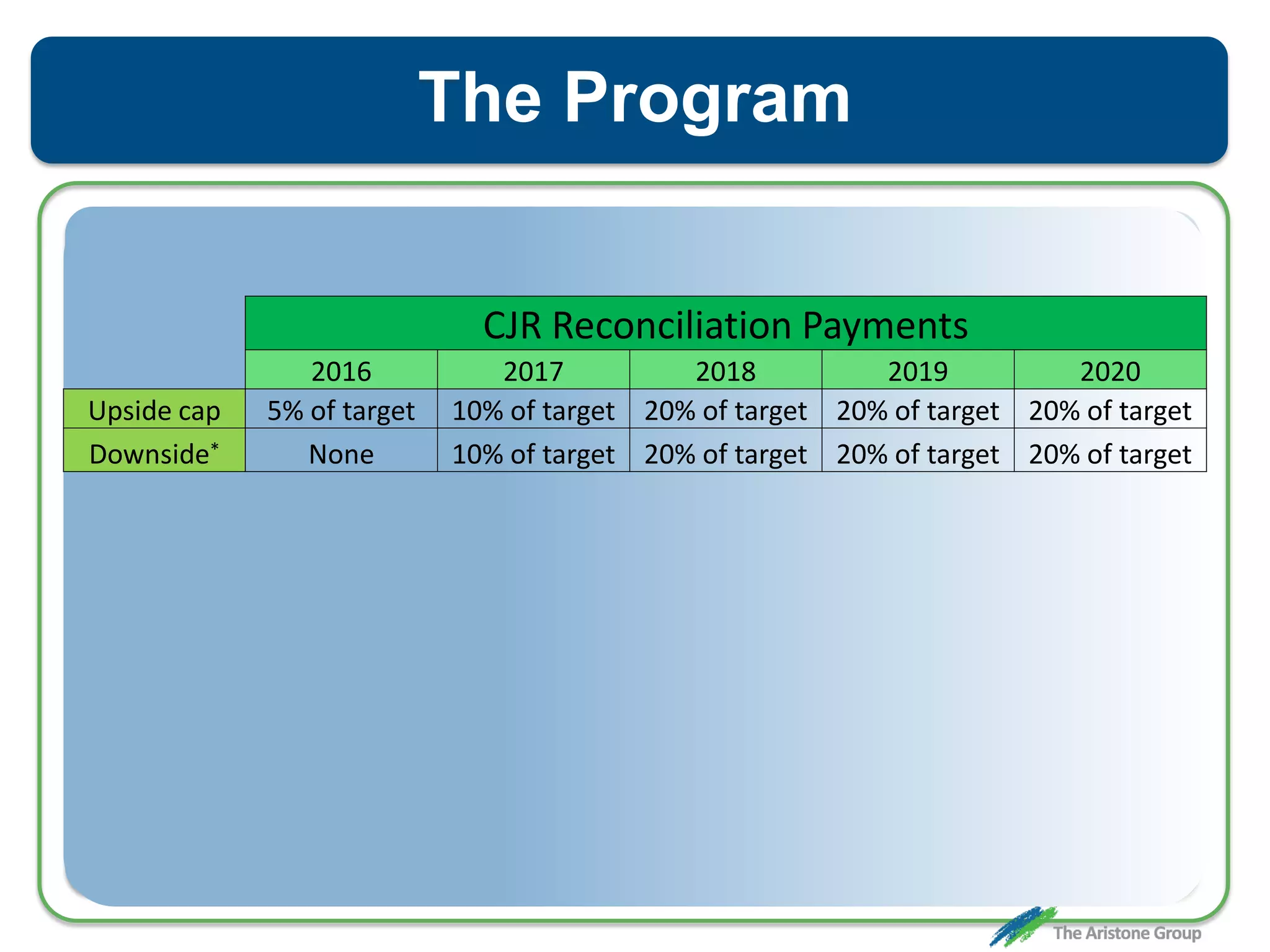
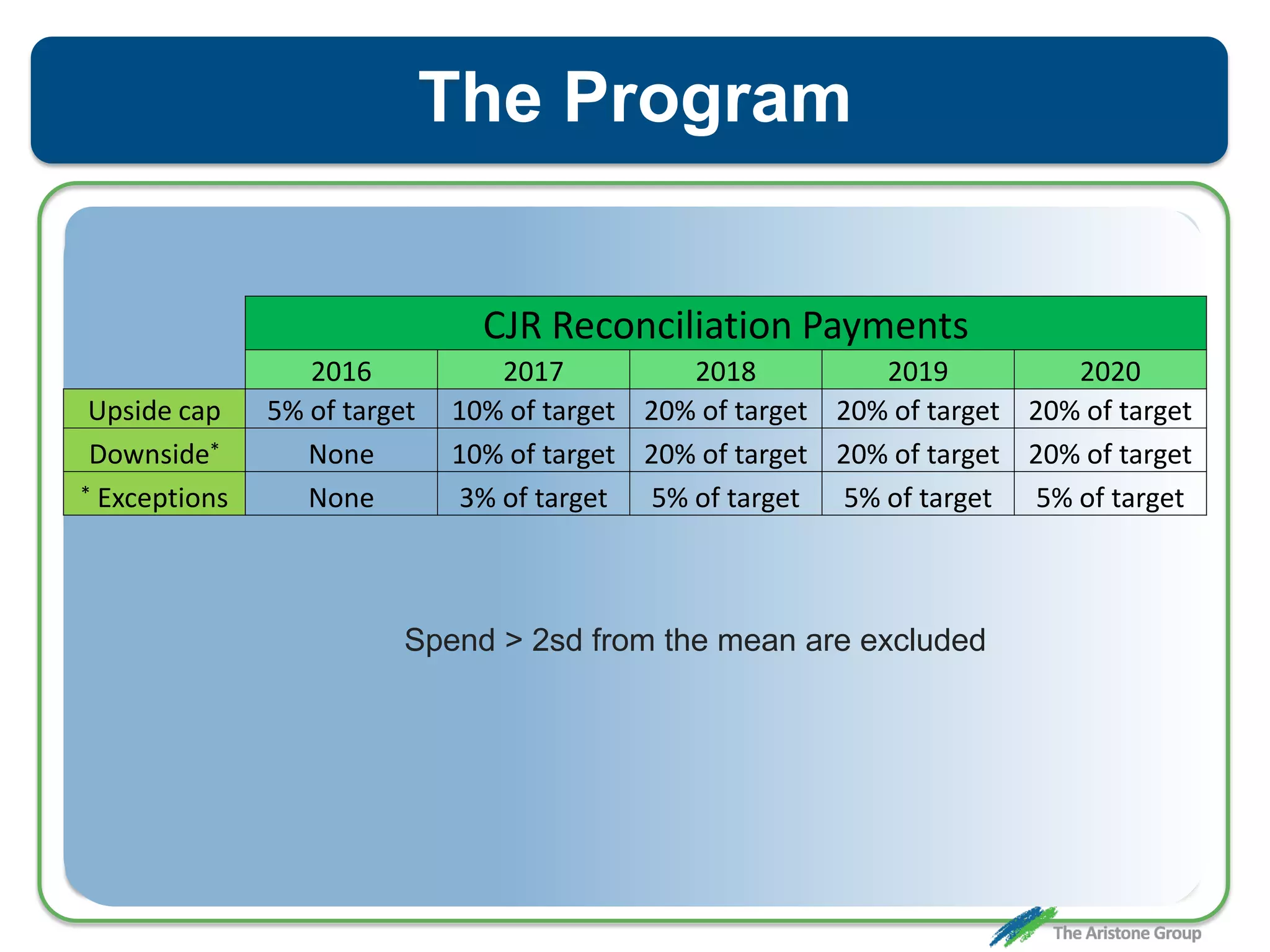

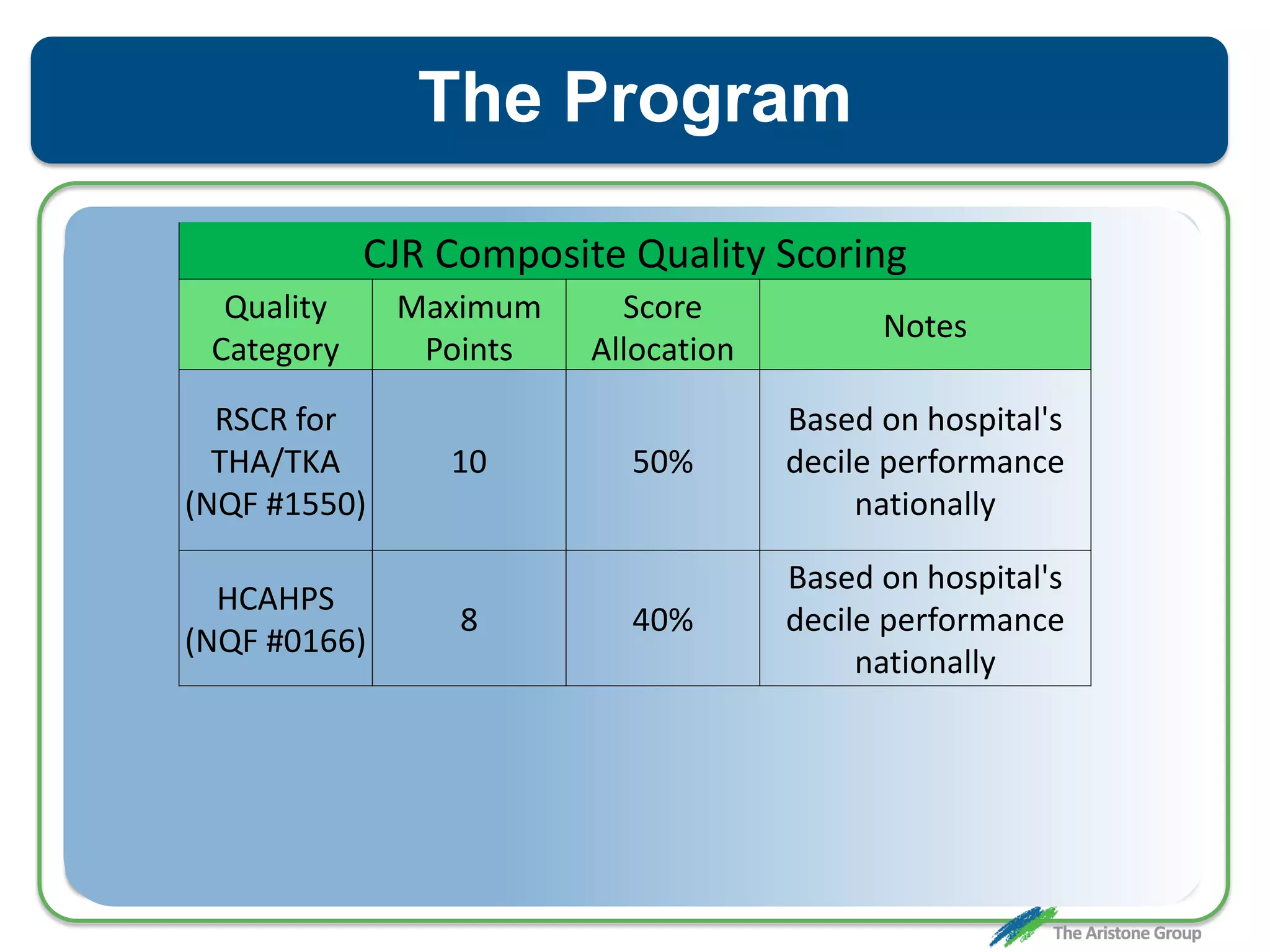
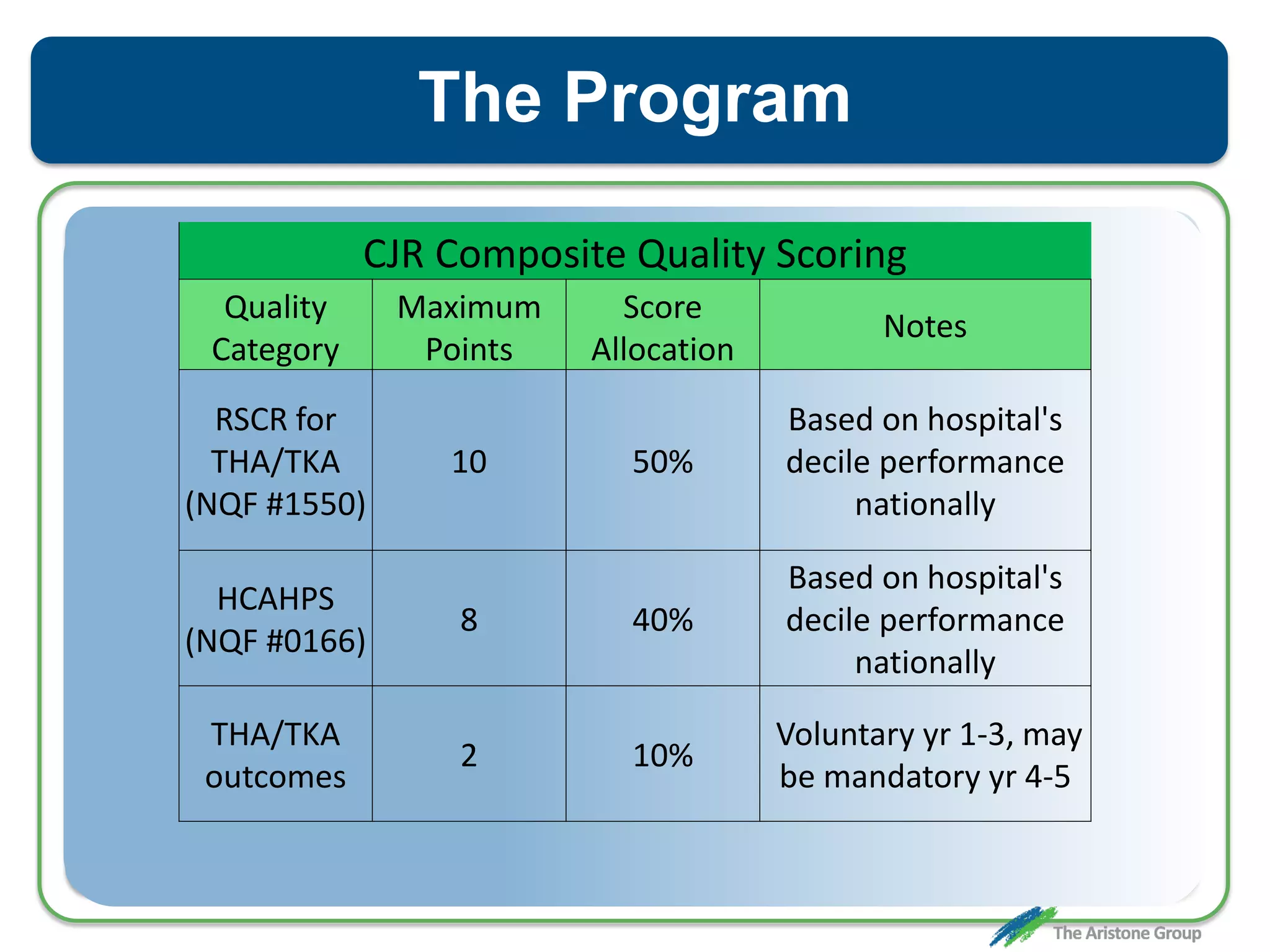
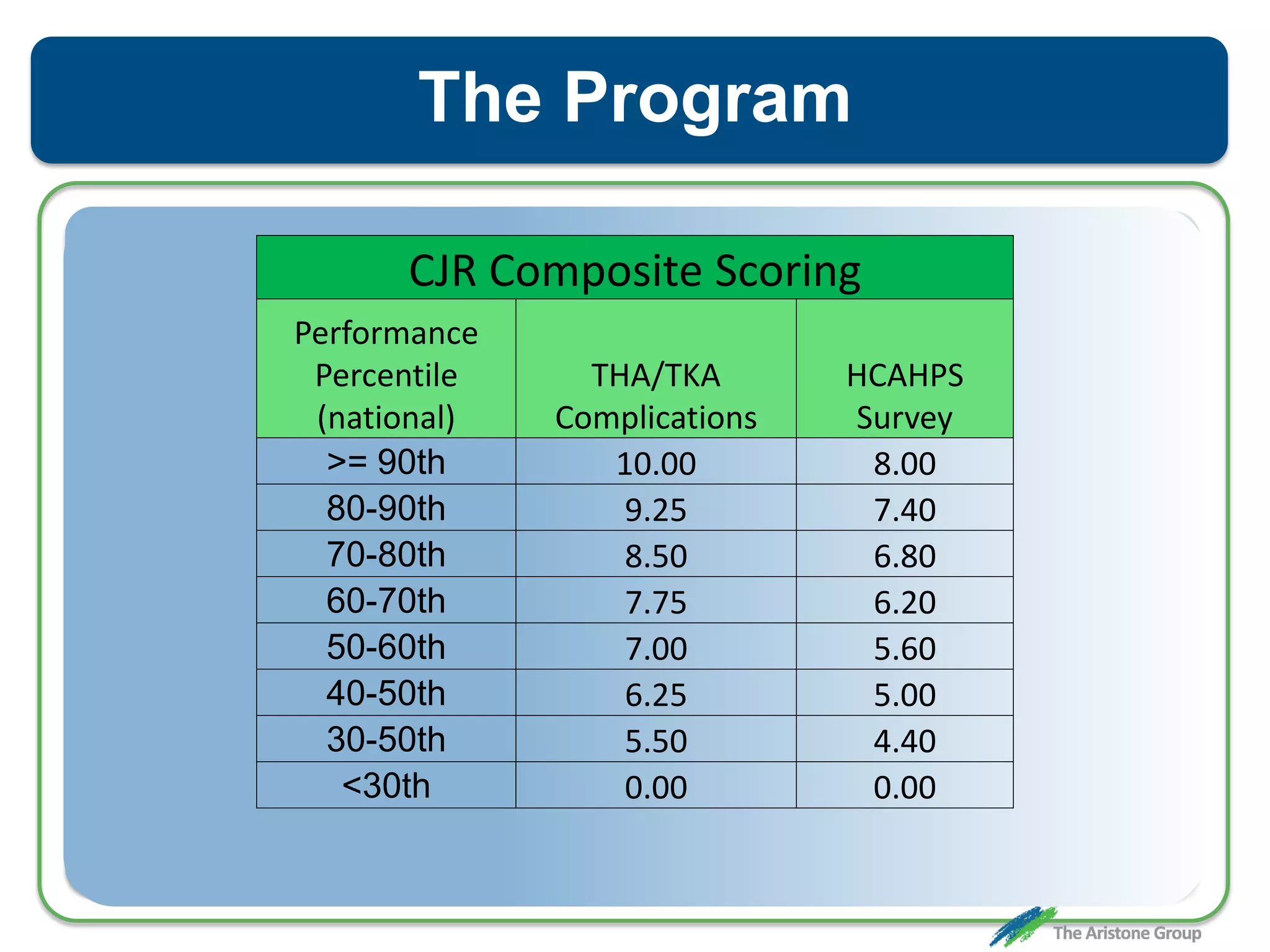

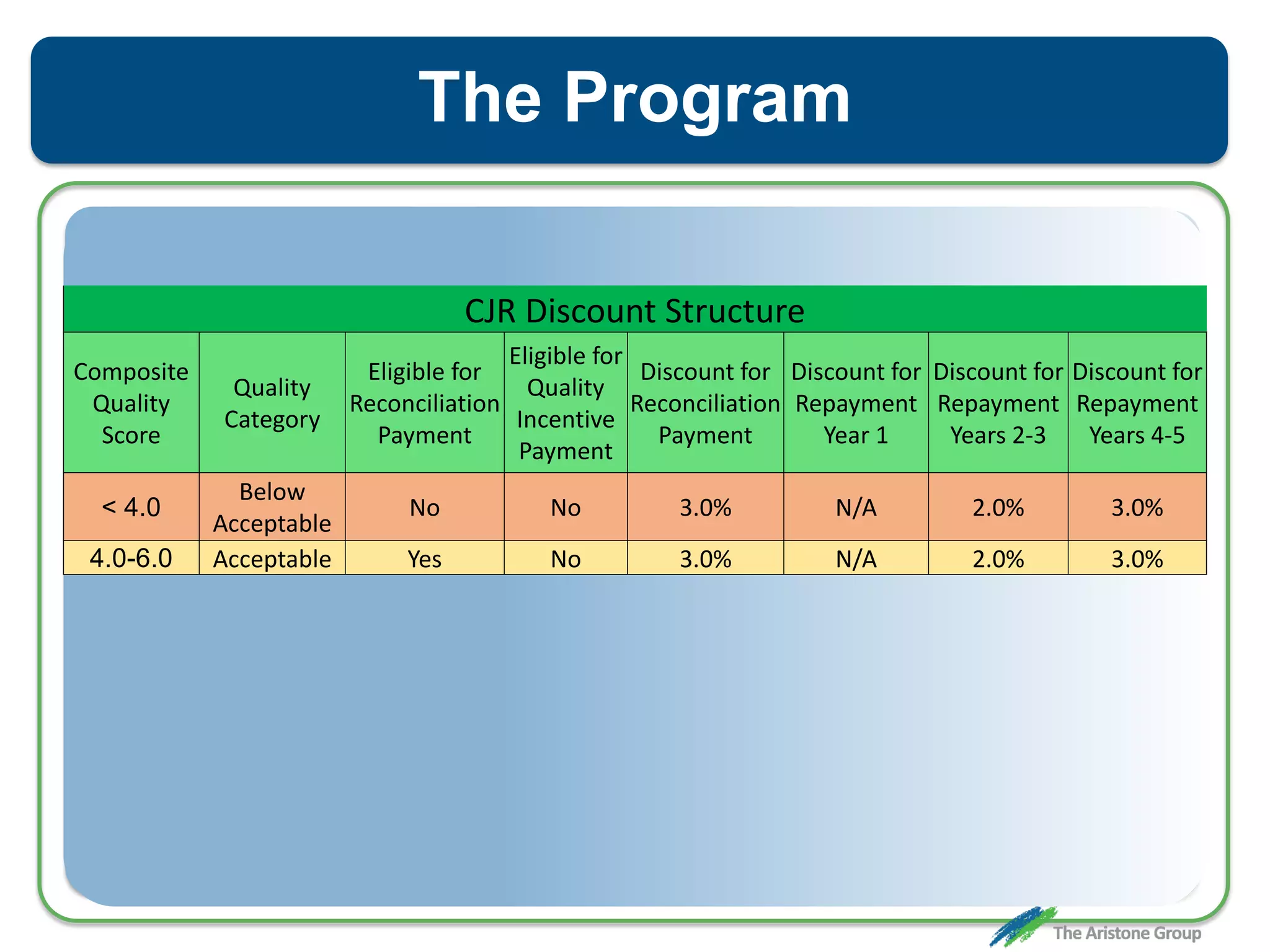
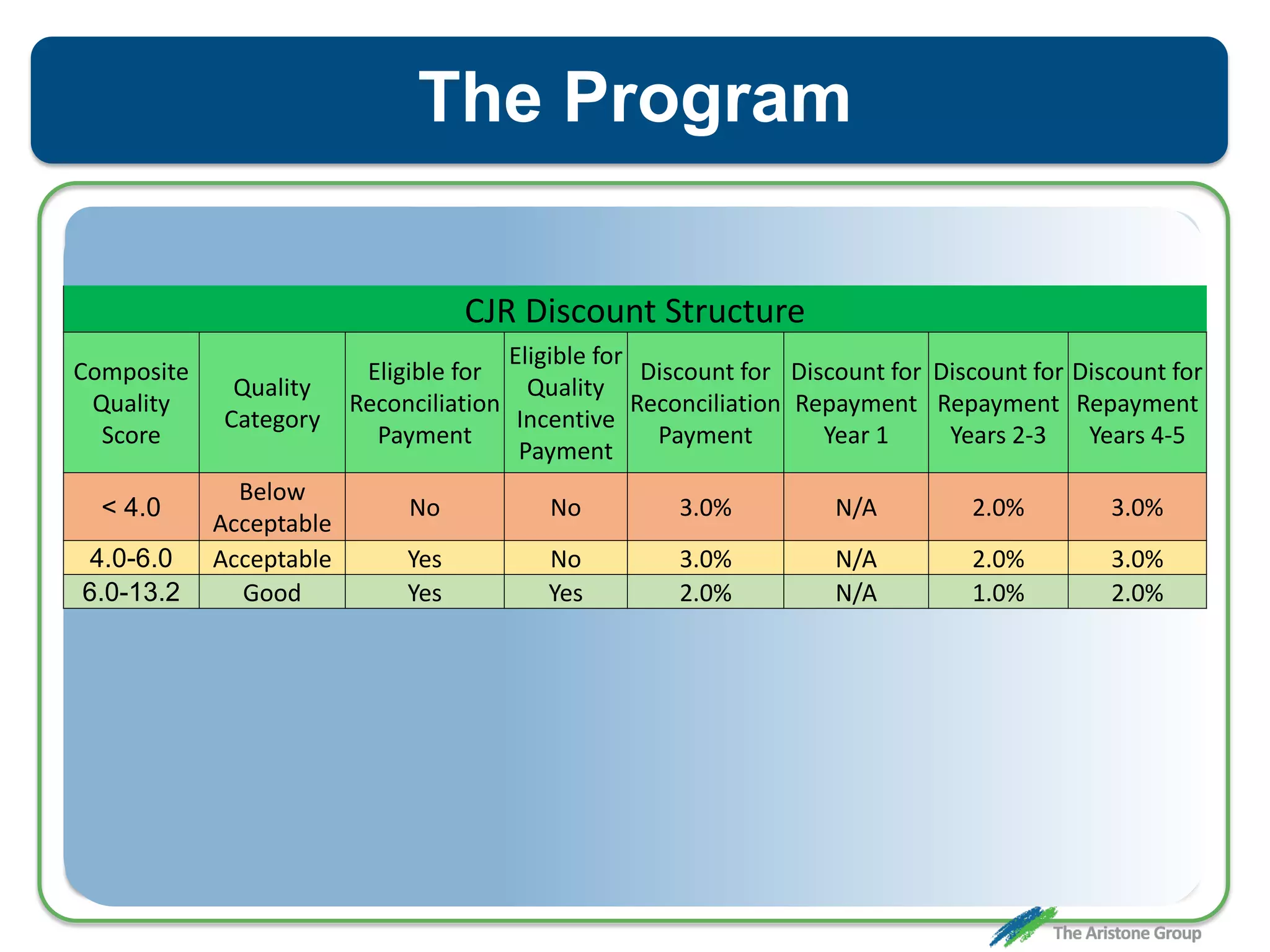
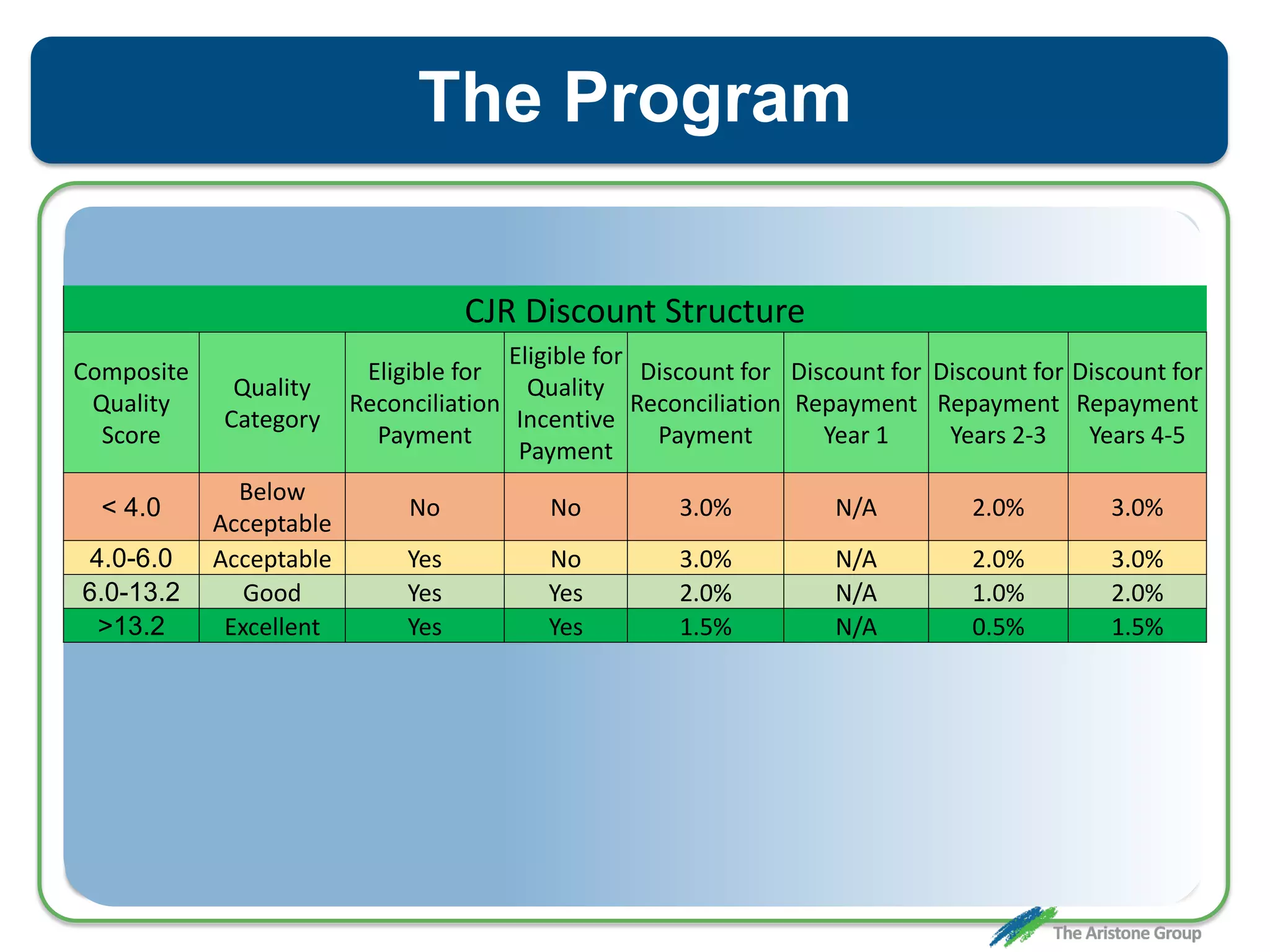



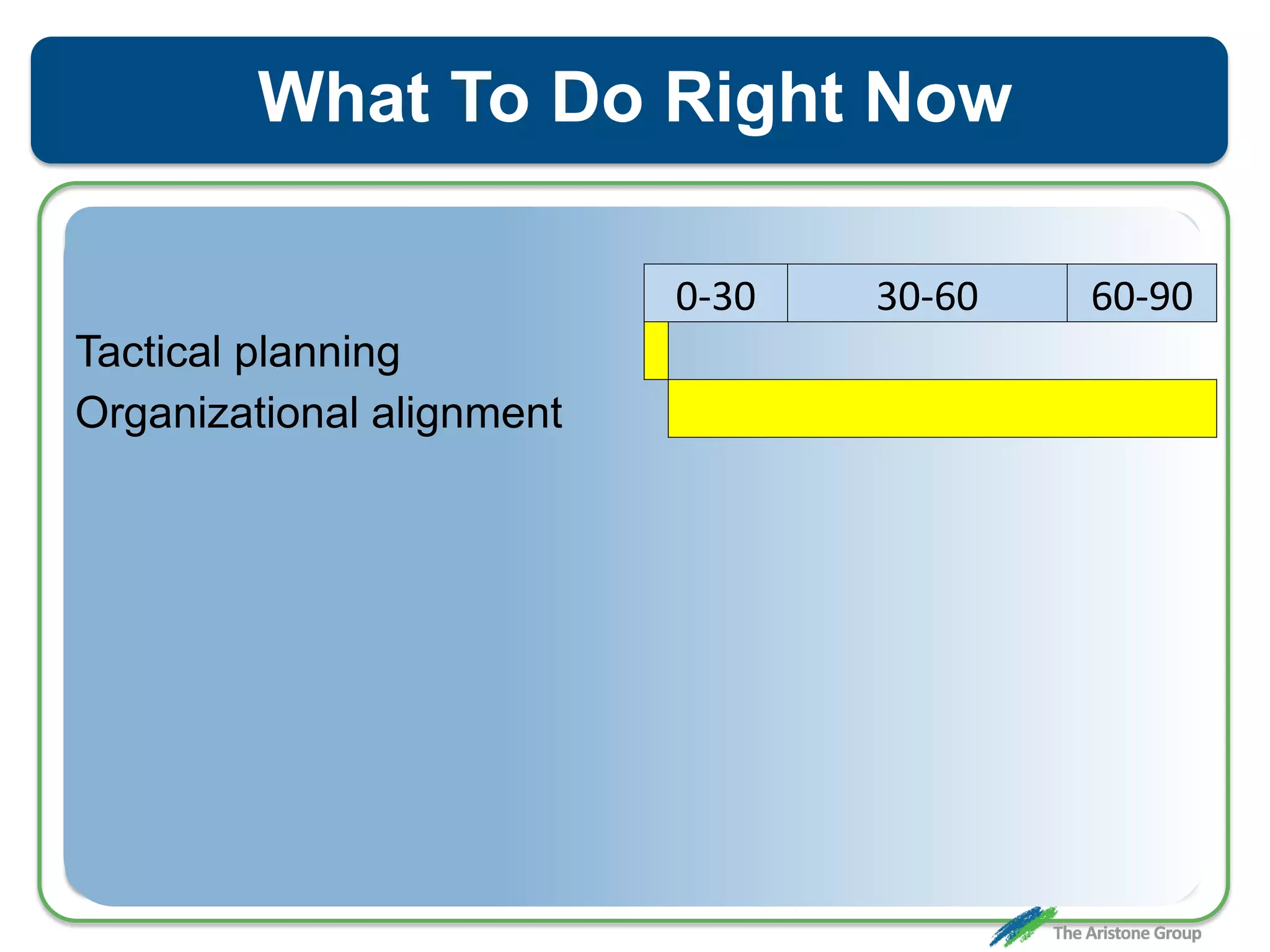

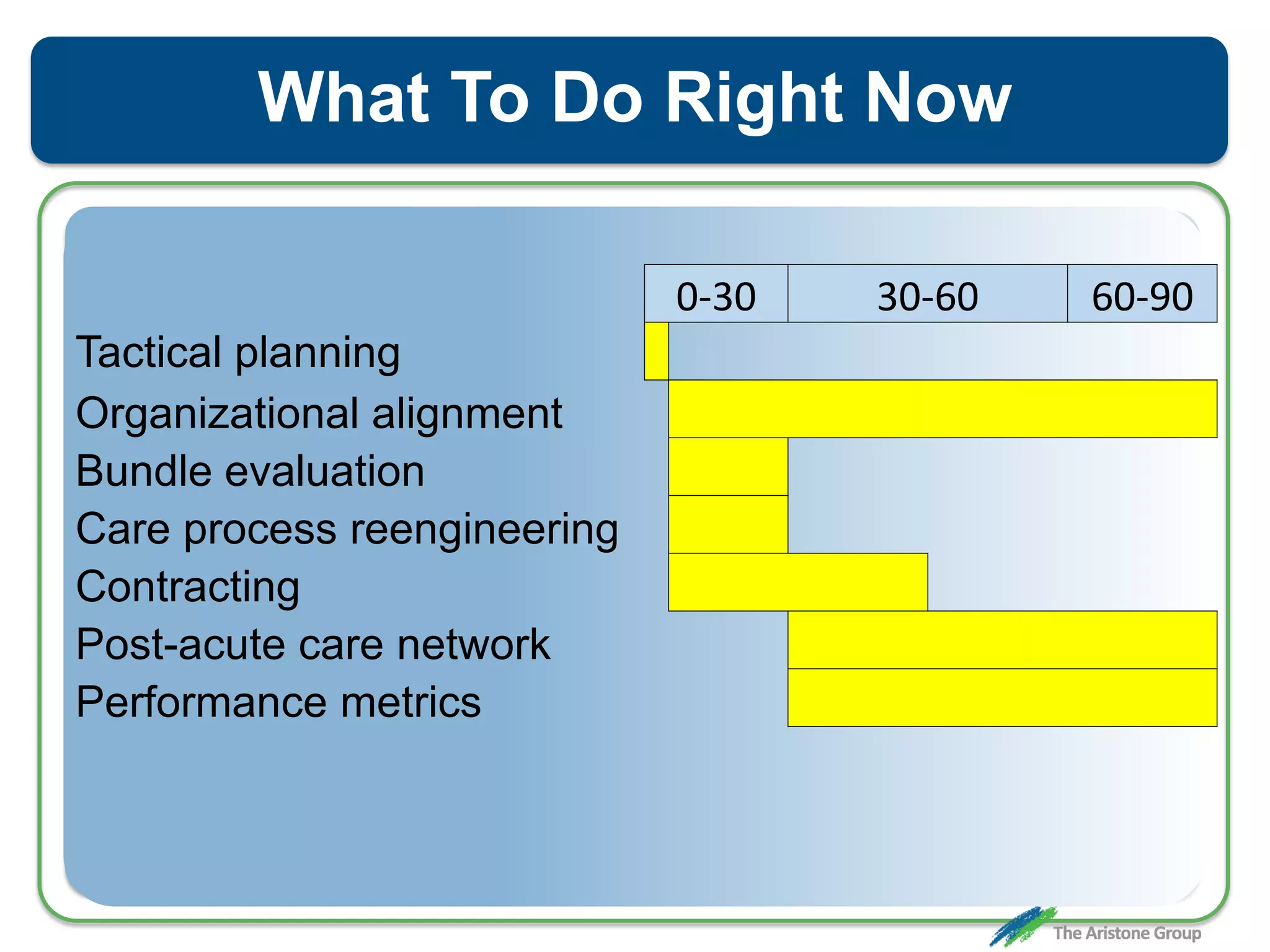





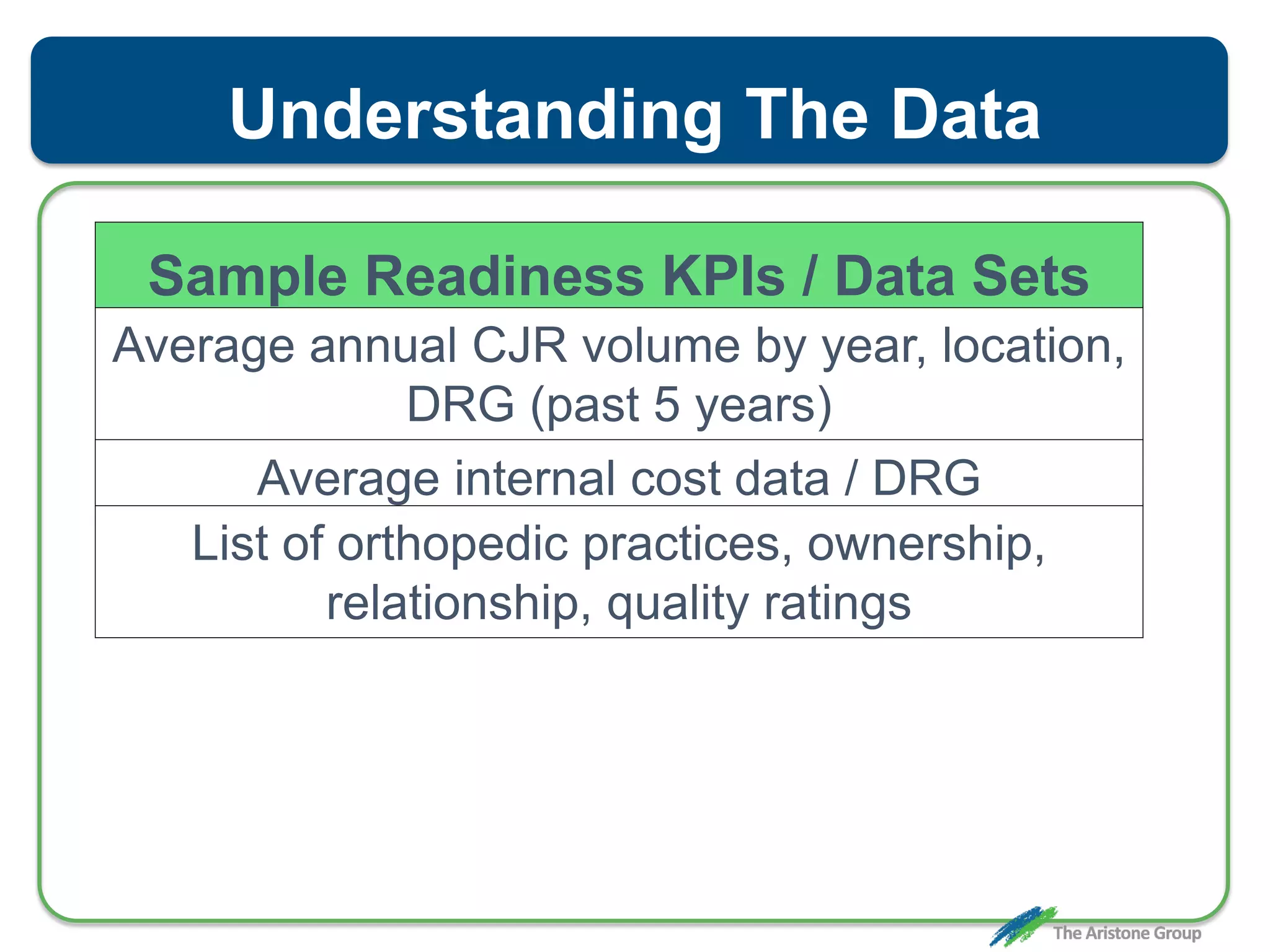
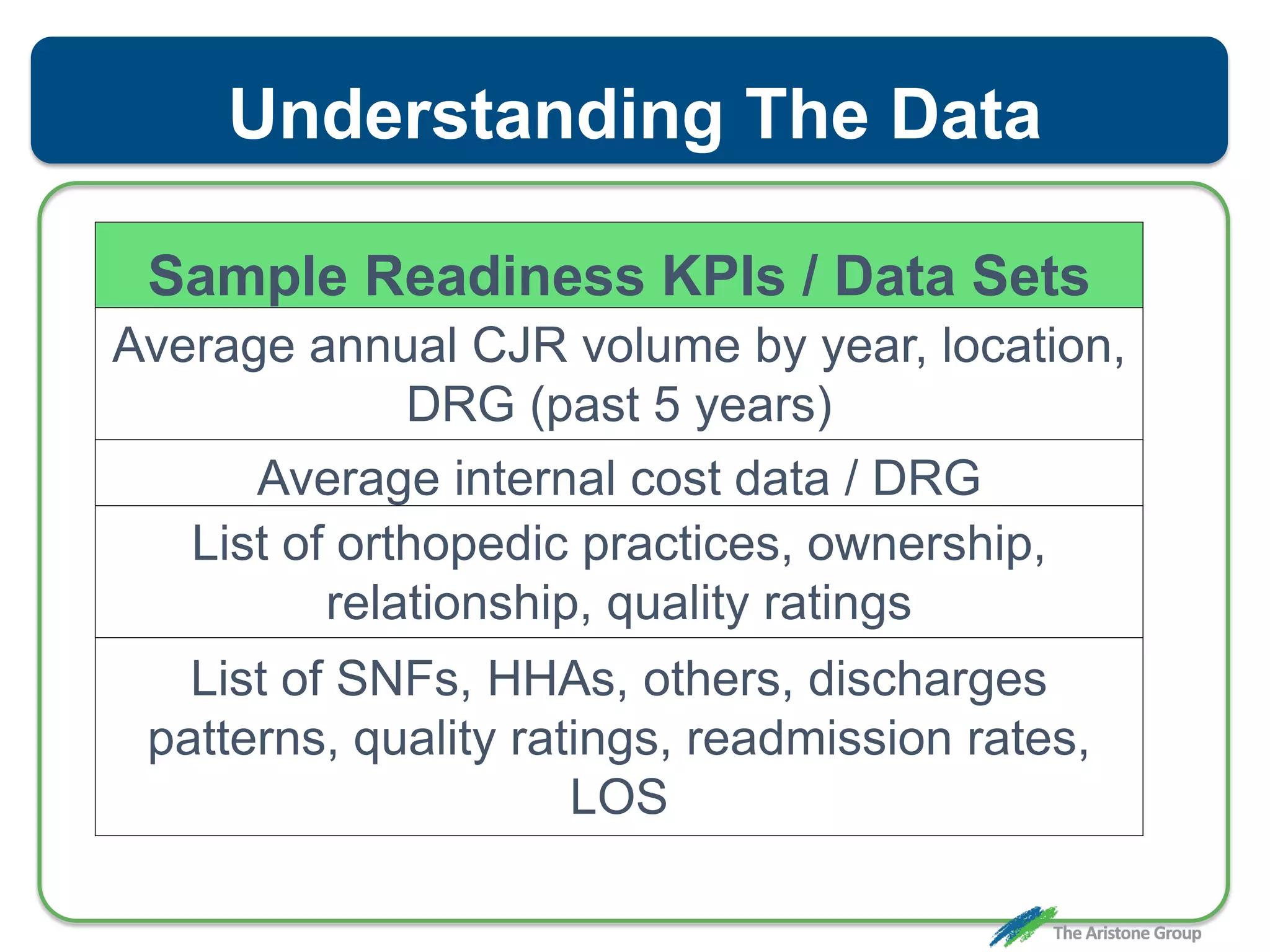






The document outlines the Comprehensive Care for Joint Replacement (CJR) program, a mandatory bundled payment initiative by Medicare for lower extremity joint procedures starting April 1, 2016. It emphasizes the importance of payer executive leadership, the need for effective post-acute care networks, and risk management strategies for successful implementation. Key details include target pricing based on regional historical data, reconciliation payments, quality scoring mechanisms, and the significance of analytics in managing the program effectively.























































































