
More Related Content
What's hot
What's hot (20)
Similar to Lv dysynchrony reporting
Similar to Lv dysynchrony reporting (20)
More from Vinayak Vadgaonkar
More from Vinayak Vadgaonkar (6)
Recently uploaded
Recently uploaded (20)
Lv dysynchrony reporting
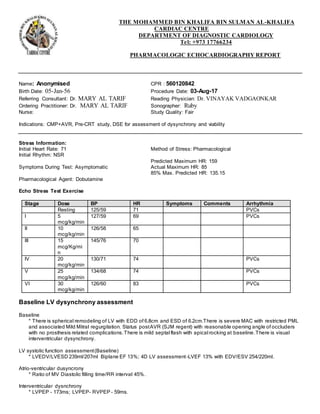
- 1. THE MOHAMMED BIN KHALIFA BIN SULMAN AL-KHALIFA CARDIAC CENTRE DEPARTMENT OF DIAGNOSTIC CARDIOLOGY Tel: +973 17766234 PHARMACOLOGIC ECHOCARDIOGRAPHY REPORT Name: Anonymised CPR : 560120842 Birth Date: 05-Jan-56 Procedure Date: 03-Aug-17 Referring Consultant: Dr. MARY AL TARIF Reading Physician: Dr. VINAYAK VADGAONKAR Ordering Practitioner: Dr. MARY AL TARIF Sonographer: Ruby Nurse: Study Quality: Fair Indications: CMP+AVR, Pre-CRT study, DSE for assessment of dysynchrony and viability Stress Information: Initial Heart Rate: 71 Method of Stress: Pharmacological Initial Rhythm: NSR Predicted Maximum HR: 159 Symptoms During Test: Asymptomatic Actual Maximum HR: 85 85% Max. Predicted HR: 135.15 Pharmacological Agent: Dobutamine Echo Stress Test Exercise Stage Dose BP HR Symptoms Comments Arrhythmia Resting 125/59 71 PVCs I 5 mcg/kg/min 127/59 69 PVCs II 10 mcg/kg/min 126/58 65 III 15 mcg/Kg/mi n 145/76 70 IV 20 mcg/kg/min 130/71 74 PVCs V 25 mcg/kg/min 134/68 74 PVCs VI 30 mcg/kg/min 126/60 83 PVCs Baseline LV dysynchrony assessment Baseline * There is spherical remodeling of LV with EDD of 6.8cm and ESD of 6.2cm.There is severe MAC with restricted PML and associated Mild Mitral regurgitation. Status postAVR (SJM regent) with reasonable opening angle of occluders with no prosthesis related complications.There is mild septal flash with apical rocking at baseline.There is visual interventricular dysynchrony. LV systolic function assessment(Baseline) * LVEDV/LVESD 239ml/207ml Biplane EF 13%; 4D LV assessment-LVEF 13% with EDV/ESV 254/220ml. Atrio-ventricular dusyncrony * Ratio of MV Diastolic filling time/RR interval 45%. Interventricular dysnchrony * LVPEP - 173ms; LVPEP- RVPEP - 59ms.
- 2. Patient Name: Anonymised CPR: 560120842 Date of Procedure: 03-Aug-17 Septal to posterior wall motion delay * 2D Anatomical M-Mode - 330ms; TDI Anatomical M-Mode - 320ms. Lateral wall post-systolic displacement * QRS to lateral wall activation - QRS to MVO = Negative value more than 100ms. Color TDI strain imaging for assessing horizontal dysynchrony/Qualitative assessment * There is visual delay between basal septal and basal lateral;Mid septum and mid lateral;Mid and basal anterior and inferior walls and significant delay betweenmid and basal posteriorand antero -septal walls. Tissue synchronisation imaging * SD Ts in 12 basal and mid LV segments - 48ms; Most delayed activationnoted basal lateral and inferolateral ; 4D Triplane TSI SD of Ts in 12 basal and mid segments - 56ms ; Most delayed activated segments are noted in lateral and inferolatreal walls. Speckle tracking strain imaging * Baseline GLPSS is -6.2% with paradoxical strain in mid to base lateral and inferior walls. There is characteristic LBBB dysynchrony as noticed on strain time graphs with early septal activation pre -systole and simultaneous lateral wall pre-stretch followed by septal delayed shortening and active contraction of lateral which is predominantin late systole. There was no significant improvement after 30mics of DSE protocol. Post DSE GLPSS is -5.6%.But there is improvement in lateral wall segmental strain. There is increased mechanical dispersioncompared to baseline. Low dose DSE for viability * There is improvement in contractility compared to baseline in basal lateral,basal inferior,mid lateral,apical septum and basal inferolatreal segments. There is no scar noted. LDDSE for Septal flash and apical rocking * There is increased septal flash and apical rocking at 30mics of dobutamine suggestive of stress induced dysynchrony. Contractile reserve.LVEF/SV * There is improvement in LVEF from 13% to 24% and Stroke volume reduced significantly from 76ml to 21ml. LBBB deformation pattern * There is type 2 LBBB deformation pattern on speckle tracking imaging with with early pre -systolic shortening with reduced shortening till the end of systole with evidence of post systolic shortening. Low dose DSE report REST ECG: True LBBB ECHO: There is spherical remodeling of LV wth EDD of 6.8cm and ESD of 6.2cm.There is severe MAC with restricted PML and associated Mild Mitral regurgitation. Status post AVR (SJM regent) with reasonable opening angle of occluders with no prosthesis related complications.There is mild septal flash with apical rocking at baseline. There is visual interventricular dysynchrony. PEAK : ECG : Sinus Tachycardia, no significant ST-T changes with multifocal PVCs ECHO : There is improvement in contrcatility compared to baseline in basal lateral,basal inferior,mid lateral,apical septum and basal inferolatreal segments.There is no scar noted.There is increased septal flash and apical rocking at 30mics of dobutamine suggestive of stress induced dysynchrony.There is improvement in LVEF from 13% to 24% and Stroke volume reduced significantly from 76ml to 21ml.
- 3. Patient Name: Anonymised CPR: 560120842 Date of Procedure: 03-Aug-17 Conclusions: Pre-CRT study with LDDSE for assessment of contractile reserve. 1. LV function assesment Biplane Simpson,s method LVEF 13% ; LVEDV/LVESV 239/207ml ; LVEDD/LVESD 6.8/6.2cm 4D LV assessment LVEF 12%; LVEDV/LVESV 254/220ml 2. Atrio-Ventricular dysynchrony * Ratio of MV Diastolic filling time/RR interval 45% 3. Interventricular dysynchrony * LVPEP - 173ms; LVPEP- RVPEP - 59ms. 4. Intraventricular dysynchrony # Septal to posterior wall motion delay 2D Anatomical M-Mode - 330ms; TDI Anatomical M-Mode - 320ms. #Lateral wall post-systolic displacement QRS to lateral wall wall activation - QRS to MVO = Negative value more than 100ms. #Color TDI strain imaging for assessing horizontal dysynchrony/Qualitative assessment There is visual delay between basal septal and basal lateral;Mid septum and mid lateral;Mid and basal anterior and inferior walls and significant delay between mid and basal posterior and antero-septal walls. #Tissue synchronisation imaging SD Ts in 12 basal and mid LV segments - 48ms; Most delayed activation noted basal lateral and inferolateral ; 4D Triplane TSI SD of Ts in 12 basal and mid segments - 56ms ; Most delayed activated segments are noted in latreal and inferolatreal walls. #Speckle tracking strain imaging Baseline GLPSS is -6.2% with paradoxical strain in mid to base lateral and inferior walls.There is charecteristic LBBB dysynchrony as noticed on strain time graphs with early septal activation pre-systole and simultaneous lateral wall pre-strech followed by septal delayed shortening and and active contraction of latreal which is predominant in late systole. There was no significant improvement after 30mics of DSE protocol.Post DSE GLPSS is -5.6%.But there is improvement in lateral wall segmental strain.There is increased mechanical dispersion compared to baseline. # LBBB deformation pattern There is type 2 LBBB deformation pattern on speckle tracking imaging with with early pre-systolic shortening with reduced shortening till the end of systole with evidence of post systolic shortening. Low dose dobutamine stress echo for viability and dysynchrony 1. There is improvement in contrcatility compared to baseline in basal lateral,basal inferior,mid lateral,apical septum and basal inferolatreal segments.There is no scar noted. 2. There is increased septal flash and apical rocking at 30mics of dobutamine suggestive of stress induced dysynchrony. 3. There is improvement in LVEF from 13% to 24% and Stroke volume reduced significantly from 76ml to 21ml.
- 4. Patient Name: Anonymised CPR: 560120842 Date of Procedure: 03-Aug-17 Reported By: Dr. VINAYAK VADGAONKAR, Mohammed Bin Khalifa Bin Sulman Al Khalifa Cardiac Centre
- 5. Patient Name: Anonymised CPR: 560120842 Date of Procedure: 03-Aug-17 Wall Motion Rest Peak Dose Key: 1=Normal, 2=Hypokinesis, 3=Akinesis, 4=Dyskinesis, 5=Aneurysmal, 6=Hyperkinetic, X=Not Visualized (Blank)=Missing
- 6. Patient Name: Anonymised CPR: 560120842 Date of Procedure: 03-Aug-17 electronically signed on 04-Aug-17 6:36:25 PM with status of Final by Dr. Vinayak