Downloaded 15 times
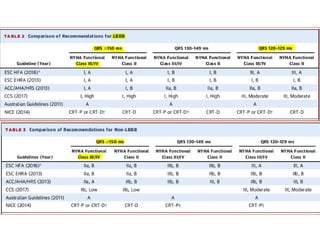
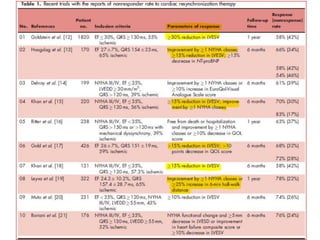
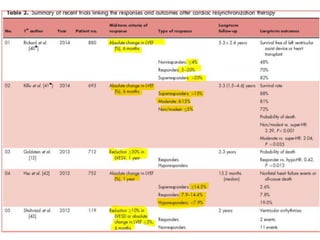
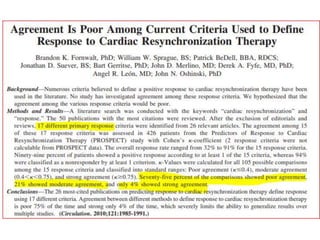

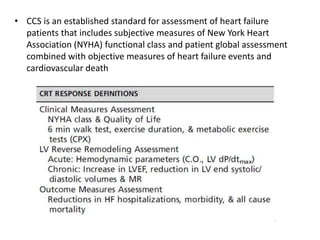
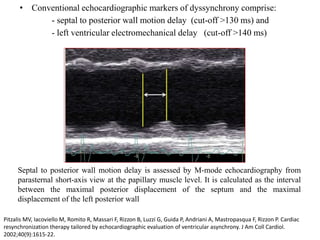
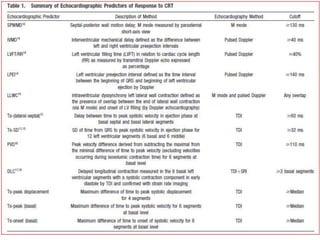
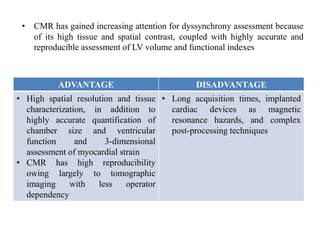
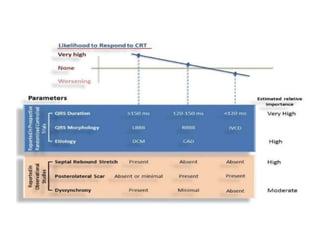

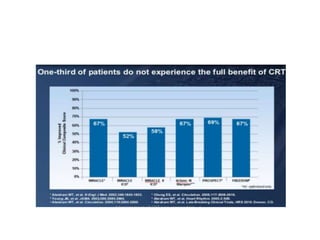
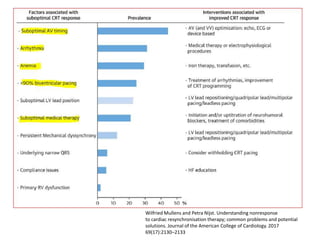
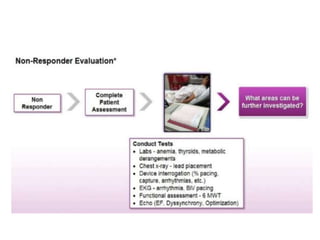
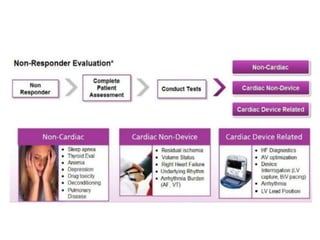
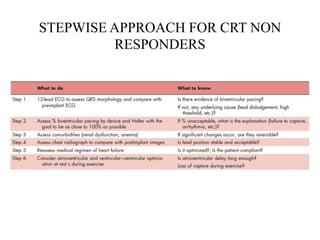
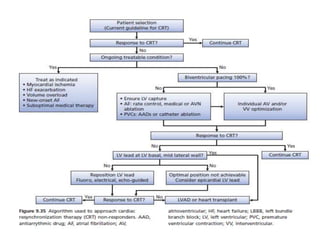
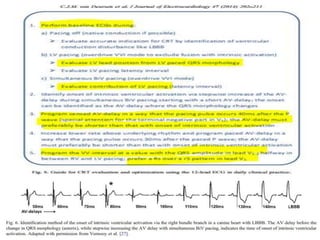
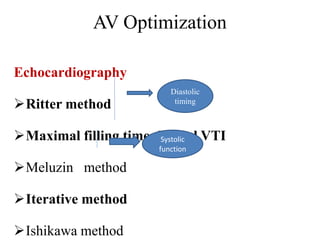
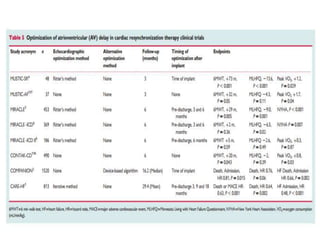
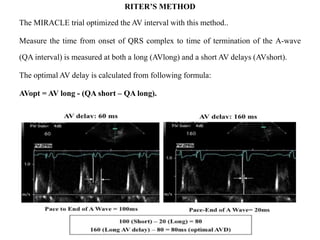
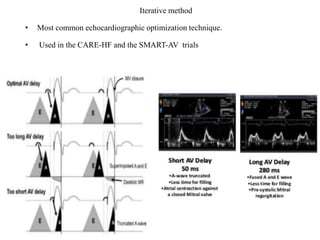
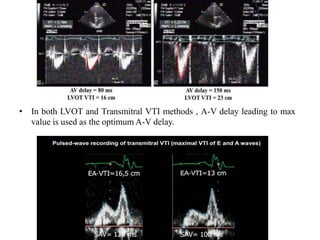

This document discusses predictors of response and non-response to cardiac resynchronization therapy (CRT). It covers several topics: 1. Electrocardiographic, echocardiographic, and imaging-based predictors of CRT response such as QRS duration, dyssynchrony parameters, apical rocking, and septal flash. 2. Steps to take for CRT non-responders, including optimizing device settings, treating arrhythmias, performing additional device-based optimization algorithms, and considering alternate lead technologies or locations. 3. Methods for optimizing atrioventricular and interventricular timing including echocardiography-based techniques and device-based algorithms. The importance of









































































