
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Basic concepts of valvular regurgitation-Echocardiography
Similar to Basic concepts of valvular regurgitation-Echocardiography (20)
Recently uploaded
Recently uploaded (20)
Basic concepts of valvular regurgitation-Echocardiography
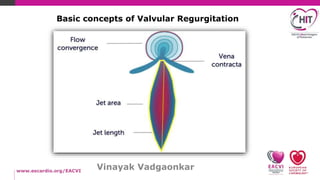
- 1. Vinayak Vadgaonkar Basic concepts of Valvular Regurgitation
- 2. How to look at any regurgitation…
- 3. ASE GUIDELINES AND STANDARDS Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation can Society of Echocardiography Developed in Collaboration with the Society for Cardiovascu Evolution of the guidelines ASE July 2003 EACVI Feb 2010 EACVI May 2013 ASE update VHD 2014 Latest April 2017….must read!!
- 4. The roadmap…. 1.2D Echo imaging • Valve structure and severity of regurgitation • Impact of regurgitation on cardiac remodelling 2.Color Doppler imaging • Jet characteristics and Jet area • Vena contracta • Flow convergence 3.Pulsed Doppler method • Forward flow • Flow reversal 4.Continous wave doppler • Spectral density • Timing of regurgitation • Time course of regurgitant velocity 5.Quantitative approaches • Effective regurgitant orifice area • Regurgitant volume • Regurgitant fraction
- 5. 2D Echo Imaging Valve structure and Severity • Etiology - Mechanism - Severity - Impact. • Normal competent leaflets have sufficient coaptation surface. • MV 8-10mm ; TV 4-9mm ; Semilunar valves few mms. • Large perforations, flail leaflet, profound retraction or marked tenting of the leaflets with coaptation gap are specific signs of s • TTE is the main modality.
- 7. Impact on Cardiac Remodelling • Cavity dilatation is directly proportional to severity and chronicity of the regurgitation. • Supportive sign/non-specific. • Multiple modulatory factors for cardiac remodelling. • Acute severe regurgitation-Normal cavity size. • Cardiomyopathies ,atrial fibrillation, ischemic LV dysfunction can contribute to remodelling of the ventricle in the presence of s • Volumes are more accurate. • Serial TTEs measurements are key.
- 8. Color Doppler Imaging What to Look for… • Origin of the regurgitant jet and size. • Spatial orientation of the regurgitant jet in the receiving chamber.
- 9. How to decode these Color flow signals… Jet characteristics and Jet area • Law of conservation of momentum. • Complex interplay between momentum, chamber constraint and minimal displayed velocity. • Sole reliance on the area of jet can be misleading. • Eccentric wall impinging jets are always underestimated. • Measure BP -driving pressure-momentum. • Non-coapting valve-Large EROA-CFM scanty because of laminar flow and decreased velocity.
- 10. Factors affecting jet area
- 11. Vena contracta What is vena contracta… • Narrowest portion of the regurgitant flow that occurs@ or immediately downstream of the regurgitant ori • High velocity laminar flow and slightly smaller than the anatomic orifice area. • CSA of VC = Measure of EROA. • Independent of flow rate and driving pressure for fixed orifice. • Independent of PRF.
- 12. How to measure vena contracta… • Linear view of the 3 components i.e. Proximal flow convergence,VC and jet area. • Beam has to be perpendicular to get maximum axial resolution and measurements. • Narrow the color sector/Zoomed view. • 2d/3D VCA. • Small errors-large % errors-misclassification of severity. MR AR
- 13. Proximal flow convergence • Located proximal to the regurgitant orifice. • Qualitative information on the location and magnitude of flow. How to assess… • Well defined small flow convergence+small jet=mild regurgitation. • Large flow convergence @ Nyquist limit of (50-70)cm/s persisting throughout the direction of flow=severe regurg TR MR FC
- 14. Pulsed Doppler Method “Alterations in forward and reversed flow” How to decode PD signals… A.Forward flow-supportive/non-specific sign. • Forward SV of the affected valve is increased. • AV valves - Increased E wave velocity;E/A ratio and short DT. • Semilunar valves - increased Peak ejection velocity,VTI forward flow and ejection time.
- 15. B.Flow reversal - Supportive /specific • Significant regurgitant volume causes flow reversal in proximal chamber. • AV valves MR -Pulmonary vein systolic flow reversal. TR - Hepatic vein systolic flow reversal • Semilunar valves AR - Prominent holodiastolic flow reversal in arch and descending aorta. PR -Diastolic flow reversal in the main or Prominent branch PAs.
- 16. How to look at flow reversal…
- 17. Continous wave Doppler What to look for…. a.Spectral density of the envelope. b.Timing of the regurgitation. c.Time course of regurgitant velocity. How to decode these CWD signals….
- 18. Spectral density • Intensity of the returned doppler signal is directly promotional to the number of RBCs reflecting the signal. • Faint ,incomplete or soft signal-trace or mild regurgitation. • Dense,complete, parabolic signal-Moderate/Severe. MR AR TR
- 19. Timing of the regurgitation • Overall assessment of physiology and hemodynamics of any regurgitation. • Majority are either holosystolic or holodiastolic,but some may occur at brief periods of time. MR AR
- 20. Time course of Regurgitant velocity • General CWD depicts parabolic shape during systole for atrioventricular valves and a trapezoid shape during diastole for semilunar valves. • For atrioventricular valves, an early peaking or cutoff sign denotes a large regurgitant wave in the respective atrium and significant regurgitation. • Rapid decay of diastolic slope in semilunar valves indicative of severe regurgitation. • Premature termination of diastolic flow -Severe Acute AR.Same does not happen in PR.
- 21. Quantitative approaches to Valvular regurgitation What to quantify… • Effective regurgitant orifice area EROA-Fundamental measure of lesion severity. • Regurgitant volume RV per beat-volume overload. • Regurgitant fraction RF - Ratio of RV to FSV specific for that regurgitation. Important note… • Careful attention should be paid whether the regurgitation covers the entire cycle i.e.holosystolic for AV valves and holodiasto • In case of partial regurgitation,Regurgitant volume is a better measure of severity.
- 22. How to quantify… There are 3 methods… 1. Quantitative pulsed doppler method. 2. Quantitative volumetric method. 3.Flow convergence method (Proximal Isovelocity Surface Area) method;PISA
- 23. Quantitative PD methods • Inflow SV - Outflow SV = Regurgitant volume. • SV = 0.785 XD2 X VTI. • Sites of calculation : LVOT,Mitral annulus and RVOT. • In the presence of single regurgitation and absence of intra-cardiac shunt,SV through the affected valve is more t Regurgitant volume = SV Regurg valve - SVcompetent valve • Regurgitant fraction = RV/SVRegurg valve. • EROA calculated from VTI of the regurgitant jet(CWD). EROA = RV/VTIRegurg jet
- 24. Mathematics
- 25. Quantitative volumetric method • Total SV ejected by ventricle in single valve regurgitation equals SV of regurgitant valve. • This method applicable mainly for left sided single valve regurgitation. • LV SV calculated by 2D volumetric method-Biplane Simpson,s method. • Forward SV measured at non-regurgitant valve;MV for AR/AV for MR. LV SV = End-diastolic volume - End-systolic volume Regurgitant volume = LV SV - SVforward EROA = RV/VTIRegurgitant jet
- 26. Flow convergence ;PISA method • The blood flow converges towards the regurgitant orifice forming concentric hemispherical shells with increasing ve • CFM images 1 of these hemispheres corresponding to the first aliasing threshold. • The aliasing threshold is when color changes from red to yellow with shift of the baseline in the direction of jet. • Radius of PISA is measured from the color doppler aliasing to VC.
- 27. PISA steps
- 28. PISA quality control a.Timing of measurements • PISA - Instantaneous flow rate -EROA obtained may not represent average regurg orifice throughout the leaking phase. • Dynamic nature of MR. • Measurement of flow and velocity should be performed in same time of regurgitation phase. • PISA representative of mean EROA measured. b.Duration of regurgitation • Partial regurgitation problems. • RV = Mean EROA X VTI obtained from densest part of the tracing. • Regurgitant volume more accurate. • Volumetric methods be used in these cases. c.Shape of the regurgitant orifice • Assumption that valvular plane from regurgitation orifice is planar with homogenous flow convergence. • Annular plane - conical. • Flow convergence not always hemispherical. • Errors in decreasing Va more;Better not to report.
- 29. PISA quality control d.Shape of the regurgitant orifice • Primary organic disease - circular orifice - overestimation of severity. • Secondary functional disease - Elliptical orifice - underestimation of severity. e.Multiple jets • Add up individual EROAs and RVs. f.3D Color flow PISA • Better assessment but limited by lower temporal and spatial resolution. g.Eccentric jets
- 30. Key message • Clinical information and Blood pressure. • Look at the valve mechanism. • Look at the chambers. • Fragment the regurgitant jet on CFM into FC-VC-Jet. • Qualitative analysis. • Quantitate as much as possible if moderate degree. • Integrate all parameters and give final judgement.