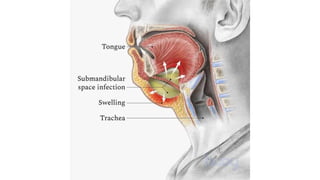
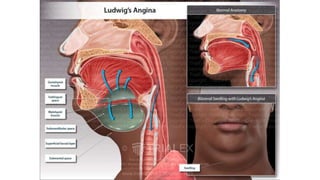
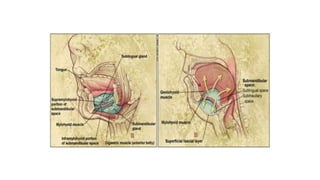
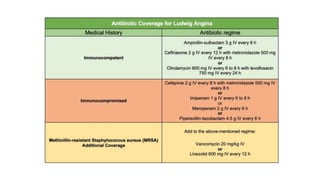
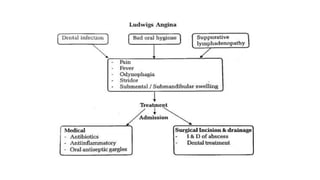
Ludwig's angina is a life-threatening infection of the soft tissues of the floor of the mouth and neck that involves three compartments - sublingual, submental, and submandibular. The infection is rapidly progressive and can lead to airway obstruction. It is most often caused by dental infections, with roots of premolars causing sublingual space infections and roots of molars causing submaxillary space infections. Treatment involves systemic antibiotics, incision and drainage of abscesses internally or externally depending on infection location, and potentially tracheostomy if the airway is endangered. Complications can include spread of infection to deeper spaces and structures as well as airway obstruction, sepsis, and aspiration pneumonia