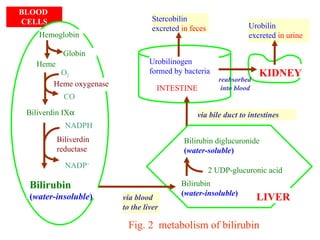
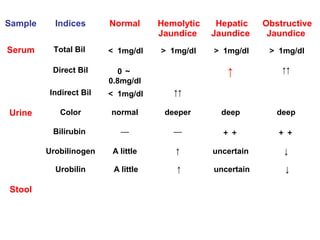
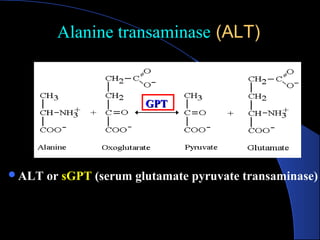
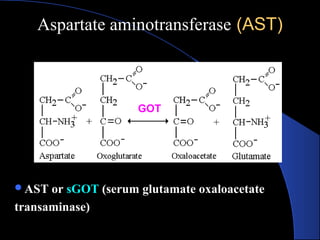
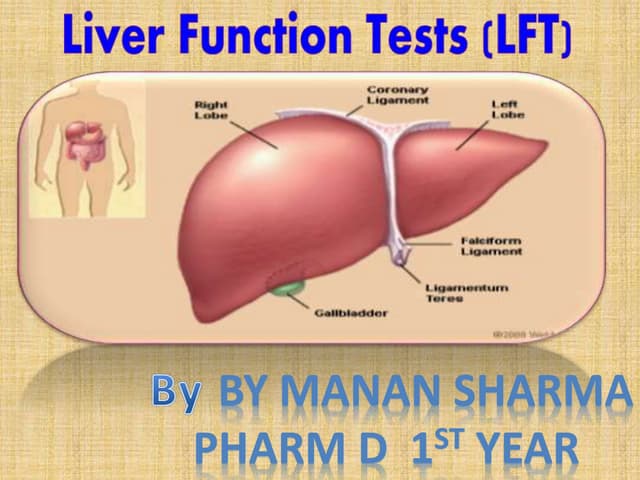
The document provides information about liver function tests (LFTs). It discusses various tests used in LFTs including bilirubin, serum enzymes, and metabolic capacity tests. Bilirubin tests examine the liver's excretory function, with elevated levels indicating issues like jaundice, liver damage, or blocked bile ducts. Serum enzyme tests like ALT, AST, and ALP measure liver injury or disease, with higher levels signaling problems. Metabolic capacity tests gauge the liver's synthetic and detoxification abilities. LFTs are important for diagnosing many liver disorders.