



![LIFE CYCLE OF PLASMODIUM
The life cycle is passed into two hosts a vertebrate ( human ) and
mosquito.
• Asexual phase in human [schizogony]: this take place in two
stages:
Exo Erythrocytic Schizogony : the infectious sporozoites are
injected from salivary gland of female Anopheles mosquitoes
during biting, into the blood stream of human.
Within 30 minutes this motile sporozoite enter liver parenchymal
cells and there it undergoes nuclear division and cytoplasmic
division and give rise to merozoites.
The parasitized liver cells ruptures and release merozoites out to
initiate Erythrocytic cycle.](https://image.slidesharecdn.com/plasmodium-240413154509-56498312/75/PLASMODIUM-PPTX-8-2048.jpg)
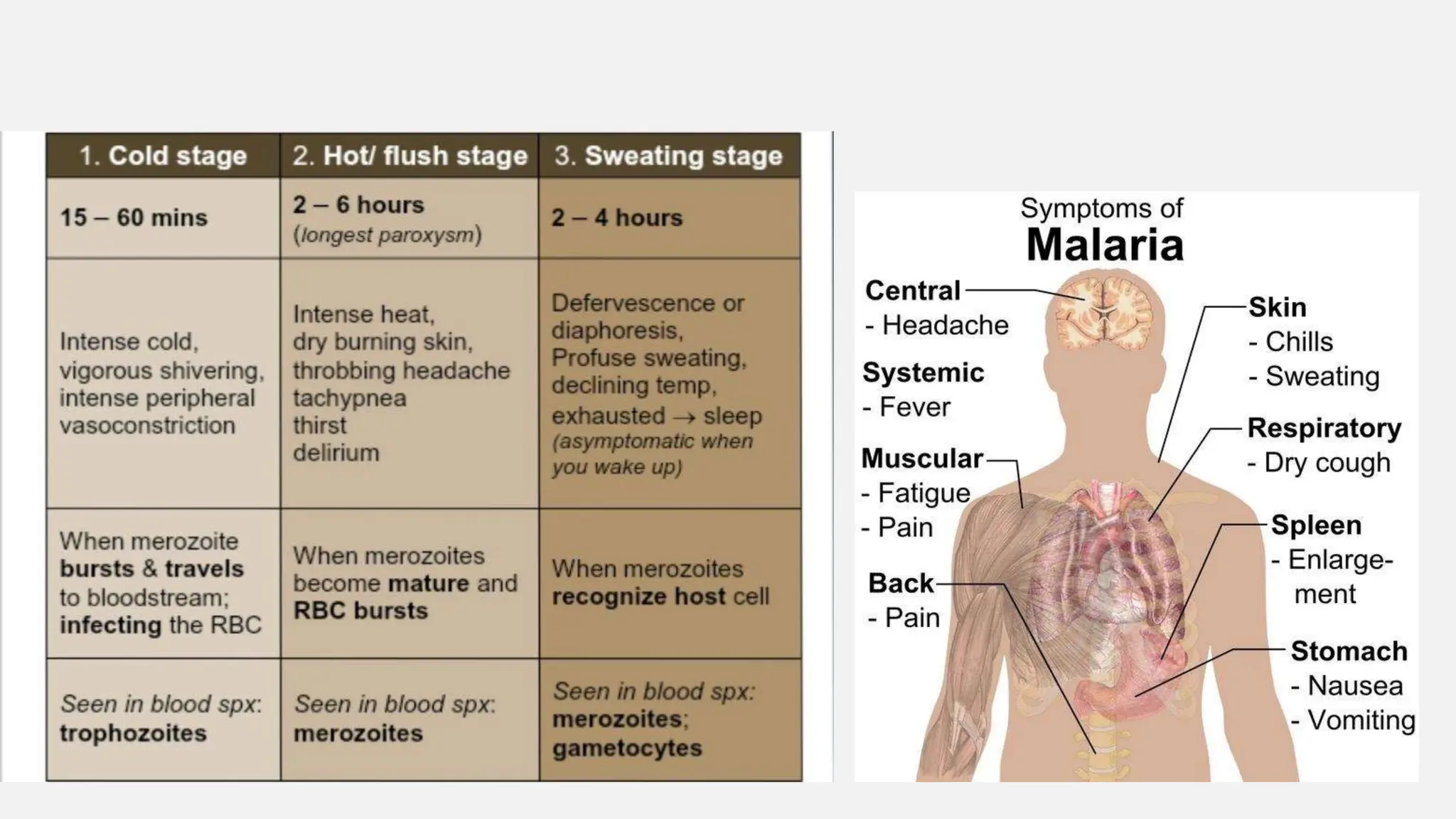
![Erythrocytic Schizogony: the released merozoties enters RBCs at this
symptoms such as fever, swelling, chills, can be seen.
Then in RBCs the merozoites develop into trophozoites and then
develop into schizonts then the cells are ruptured and re invasion to
news cells occurs.
Gametogony: some merozoites released from RBC donot undergoes
schizogony nor infect more RBCs but they develop into male and
female gametocytes which are infectious to mosquitoes.
• Sexual phase in mosquitoes [sporogony]: male and female
gametocytes are sucked in by mosquitoes during blood meal (biting)
which undergoes maturation and differentiation into microgametes
(male) and macrogametes(female).
Microgamete fertilize macrogamete producing zygote. The zygote
becomes motile and penetrates the mosquito’s gut as ookinette which
develop into oocyst.](https://image.slidesharecdn.com/plasmodium-240413154509-56498312/75/PLASMODIUM-PPTX-9-2048.jpg)



![To detect antibodies produced against malarial antigen.
• Treatments: antimalarial drugs
1.Artemisinin drug [Artemether and Artesunate combination]
2. Atovaquone
3.Doxycycline
4.Mefloquine
5.Quinine- for pregnant women
6. Primaquine
Vaccine- RTS, S/AS01 for p.falciparum in children](https://image.slidesharecdn.com/plasmodium-240413154509-56498312/75/PLASMODIUM-PPTX-17-2048.jpg)


Plasmodium are unicellular protozoan parasites that cause malaria in humans. They have a complex lifecycle involving sexual reproduction in mosquitos and asexual reproduction in human liver and blood cells. Malaria symptoms include fever, chills, and anemia. Diagnosis involves examining blood smears for parasites, and treatment involves antimalarial drugs. Prevention relies on mosquito control and use of bed nets and repellents.



































































