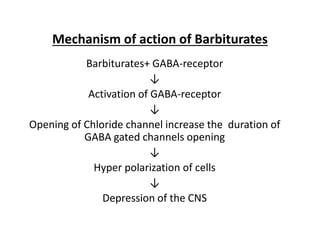
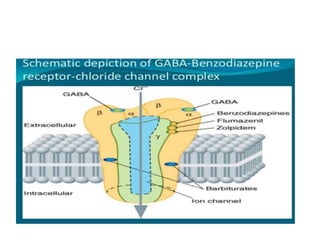
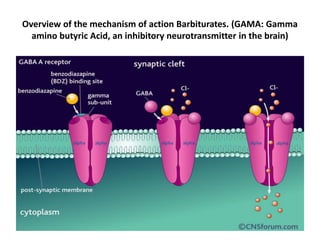
Sedative-hypnotic drugs reduce anxiety and induce sleep by depressing activity in the central nervous system. The main classes are benzodiazepines, barbiturates, and newer non-benzodiazepine agents. Benzodiazepines have largely replaced barbiturates due to their wider therapeutic index, lower risk of interactions and dependence, and the availability of antagonists. Both benzodiazepines and barbiturates work by enhancing the effects of the inhibitory neurotransmitter GABA.
















































![4._Sedative_hypnotics[1].pptx pharmacy students](https://cdn.slidesharecdn.com/ss_thumbnails/4-251117163021-acac7ad2-thumbnail.jpg?width=640&height=640&fit=bounds)




















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)