Download as PDF, PPTX


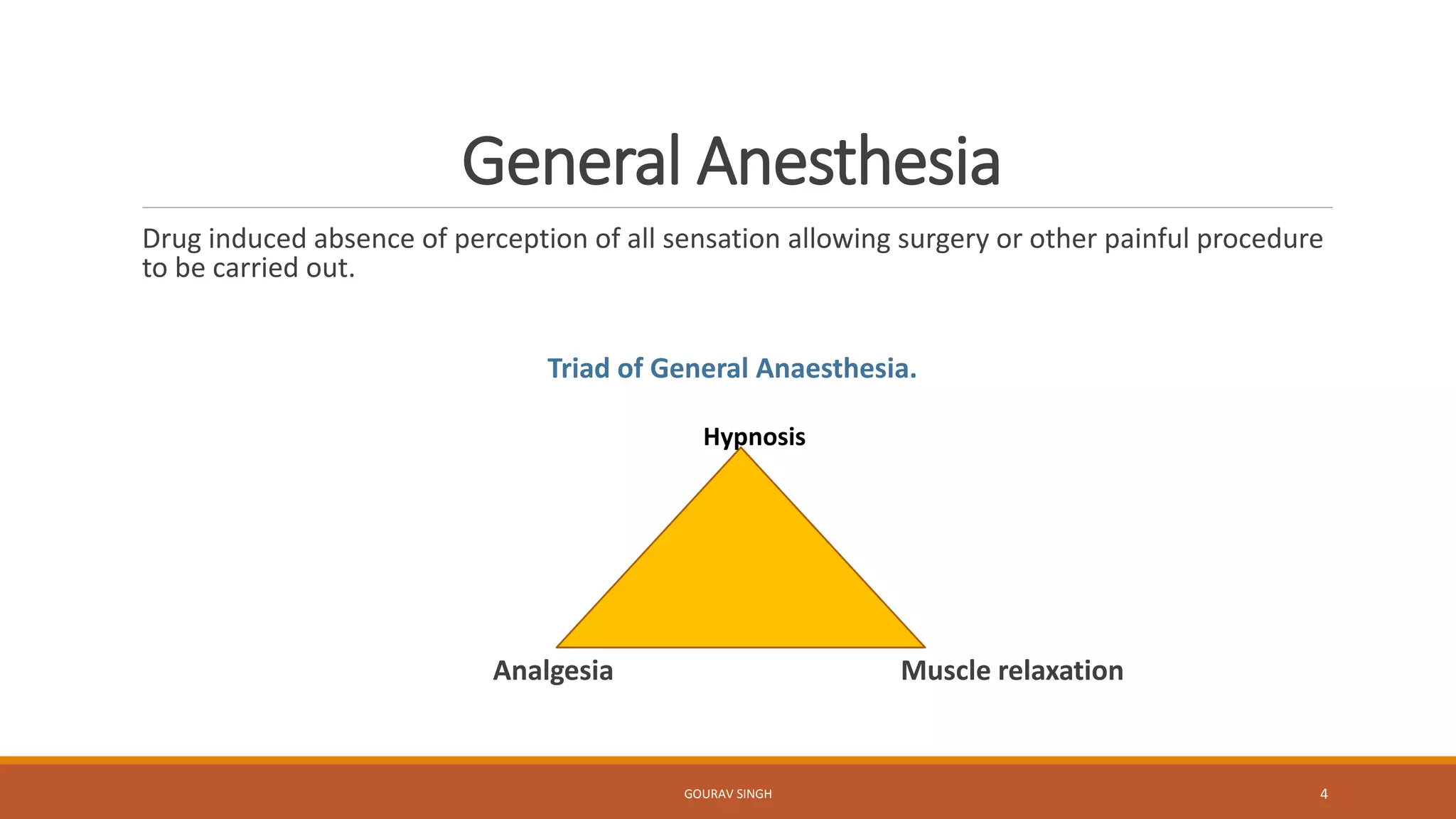

















The document discusses different aspects of anesthesia including: 1. Anesthesia refers to reversible loss of sensation and consciousness and is achieved through anesthetic agents that induce loss of pain and sensation along with loss of reflexes. 2. There are two main types of anesthesia - local anesthesia and general anesthesia. General anesthesia involves drug-induced absence of all sensation allowing surgery. 3. Anesthesia works through several stages from initial analgesia to eventual respiratory paralysis if overdosed. Proper pre-anesthesia medications are used to make the anesthesia safer and more comfortable for the patient.








![1.Hemodynamic and electrophysiology [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/1-240116072053-6f97ce28-thumbnail.jpg?width=640&height=640&fit=bounds)














































































