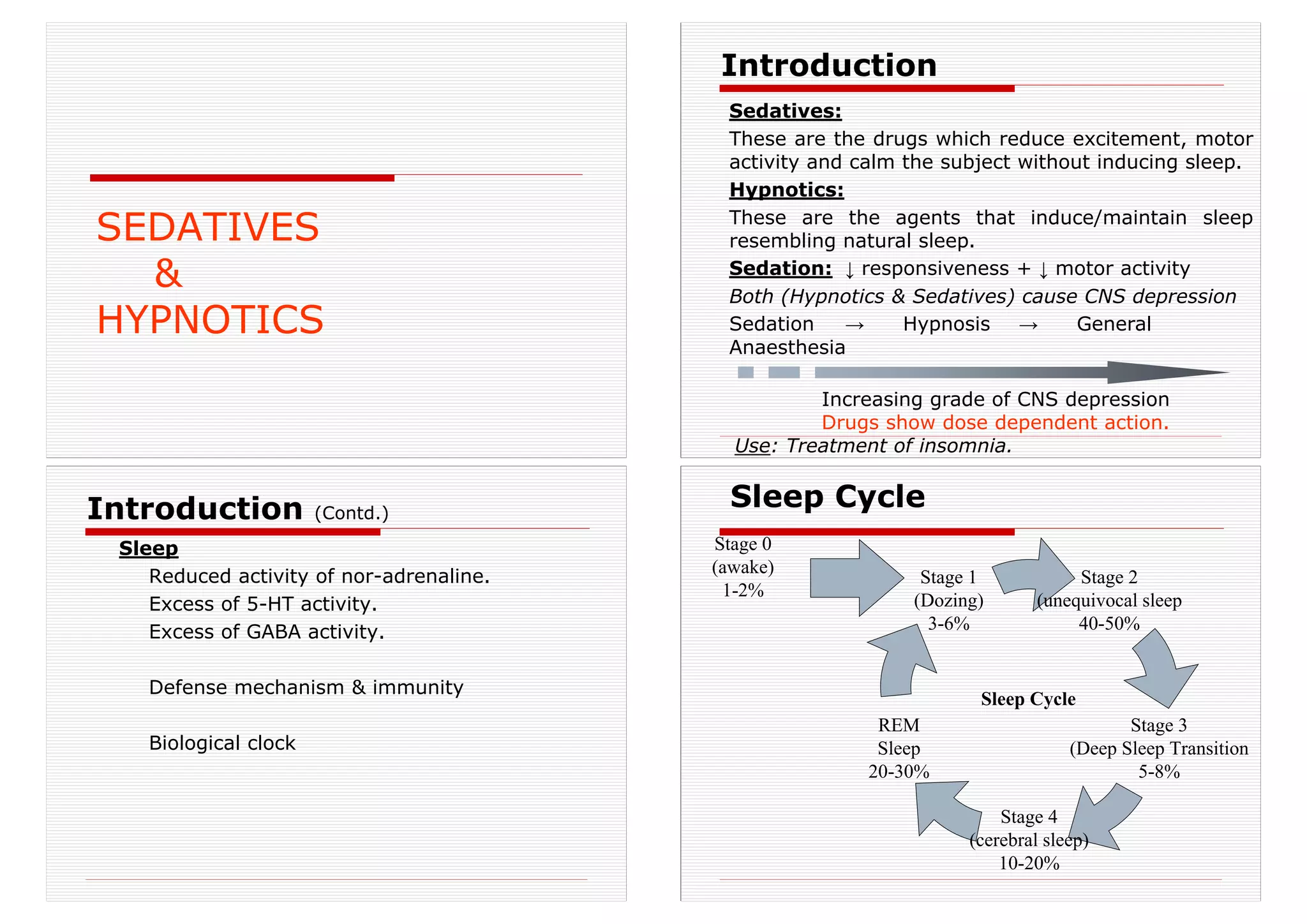
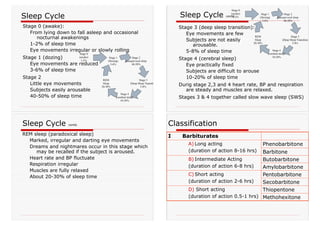
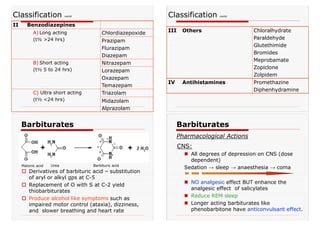
This document summarizes information about sedatives and hypnotics. It defines sedatives as drugs that reduce excitement and motor activity without inducing sleep, while hypnotics induce and maintain sleep resembling natural sleep. Both cause central nervous system depression in a dose-dependent manner, from sedation to hypnosis to general anesthesia. Common hypnotics discussed include barbiturates, benzodiazepines, chloral hydrate, and other drugs. Their mechanisms of action, pharmacokinetics, uses, side effects, and overdose treatment are concisely described.


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















