
Downloaded 10 times





![Meconium :
• The term Meconium derives from ‘meconium-arion’, meaning
"opium-like", in reference either to its tarry appearance or to
Aristotle's belief that it induces sleep in the fetus.[2]
• Initial fecal material is meconium which is passed within 24 hrs
after birth.
• Unlike later feces, meconium is composed of materials ingested
during the time the infant spends in the uterus: intestinal epithelial
cells, lanugo, mucus, amniotic fluid, bile, and water. Meconium is
sterile, unlike later feces, & is viscous and sticky like tar, and has
no odor. It should be completely passed by the end of the first few
days of life, with the stools progressing toward yellow (digested
milk).](https://image.slidesharecdn.com/lecture-4-200917042956/85/Lecture-4-Normal-Newborn-45-320.jpg)
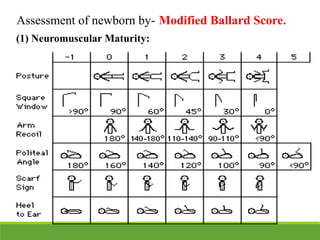
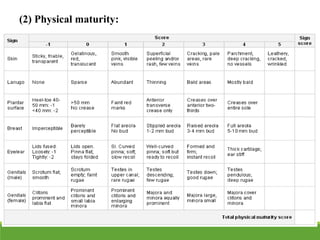
This document provides an overview of the normal newborn period, defining key stages from birth to 28 days, including early and late neonatal periods. It emphasizes the significant physiological changes a newborn undergoes at birth and details assessments such as the Apgar score for evaluating newborn health. Additionally, it describes various physical characteristics and common conditions observed in newborns, along with vital statistics and measures.























































































