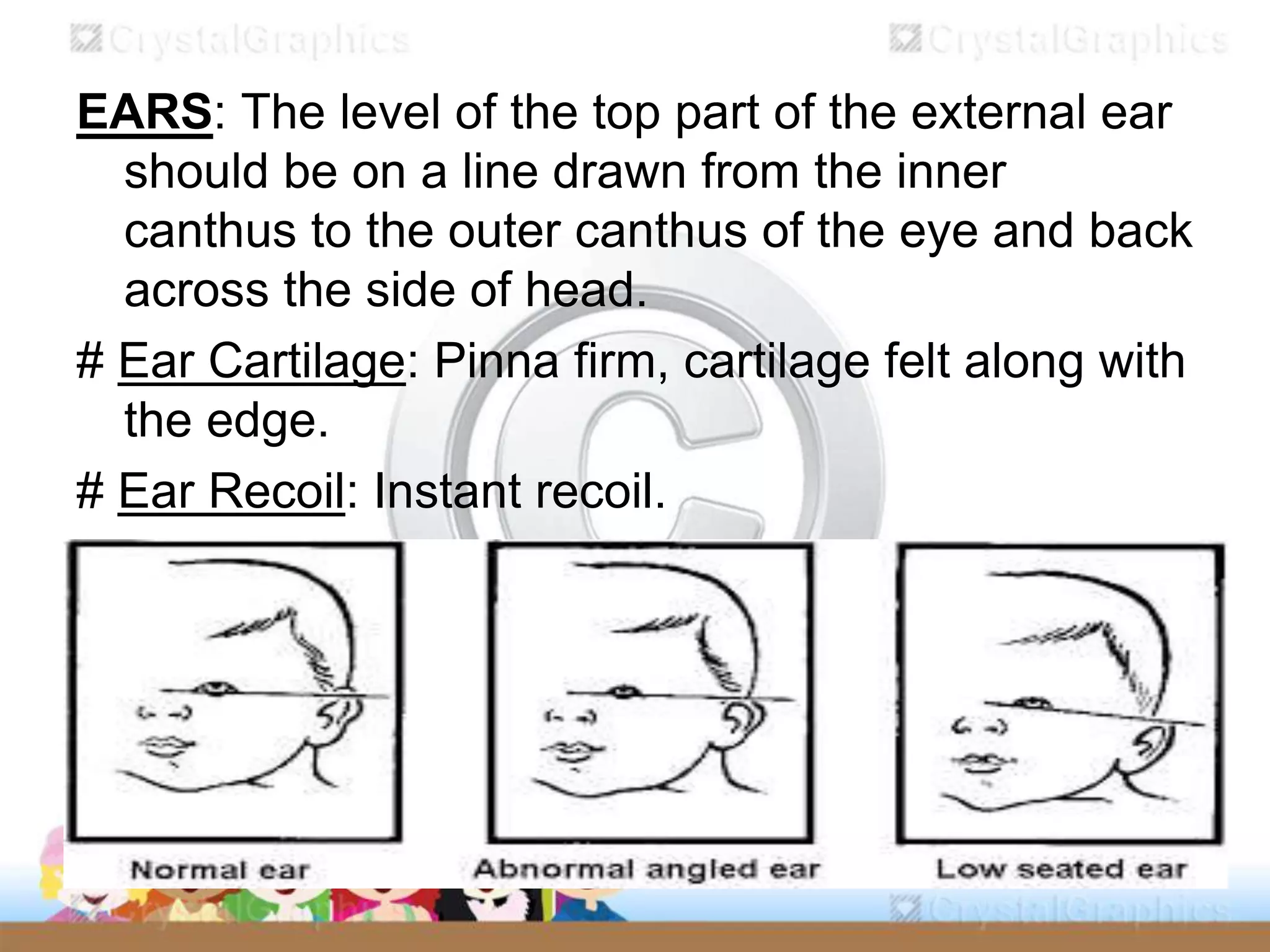
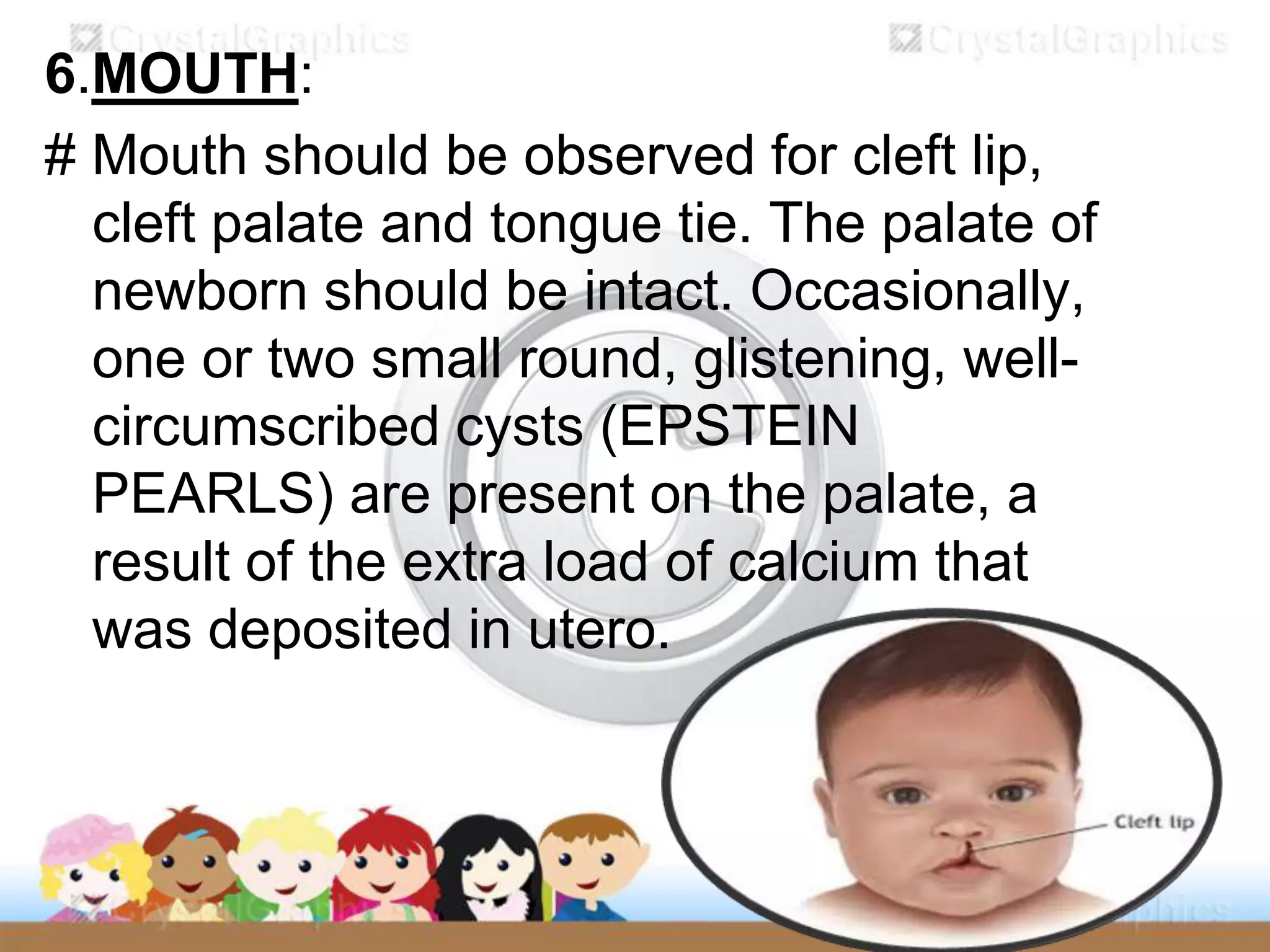
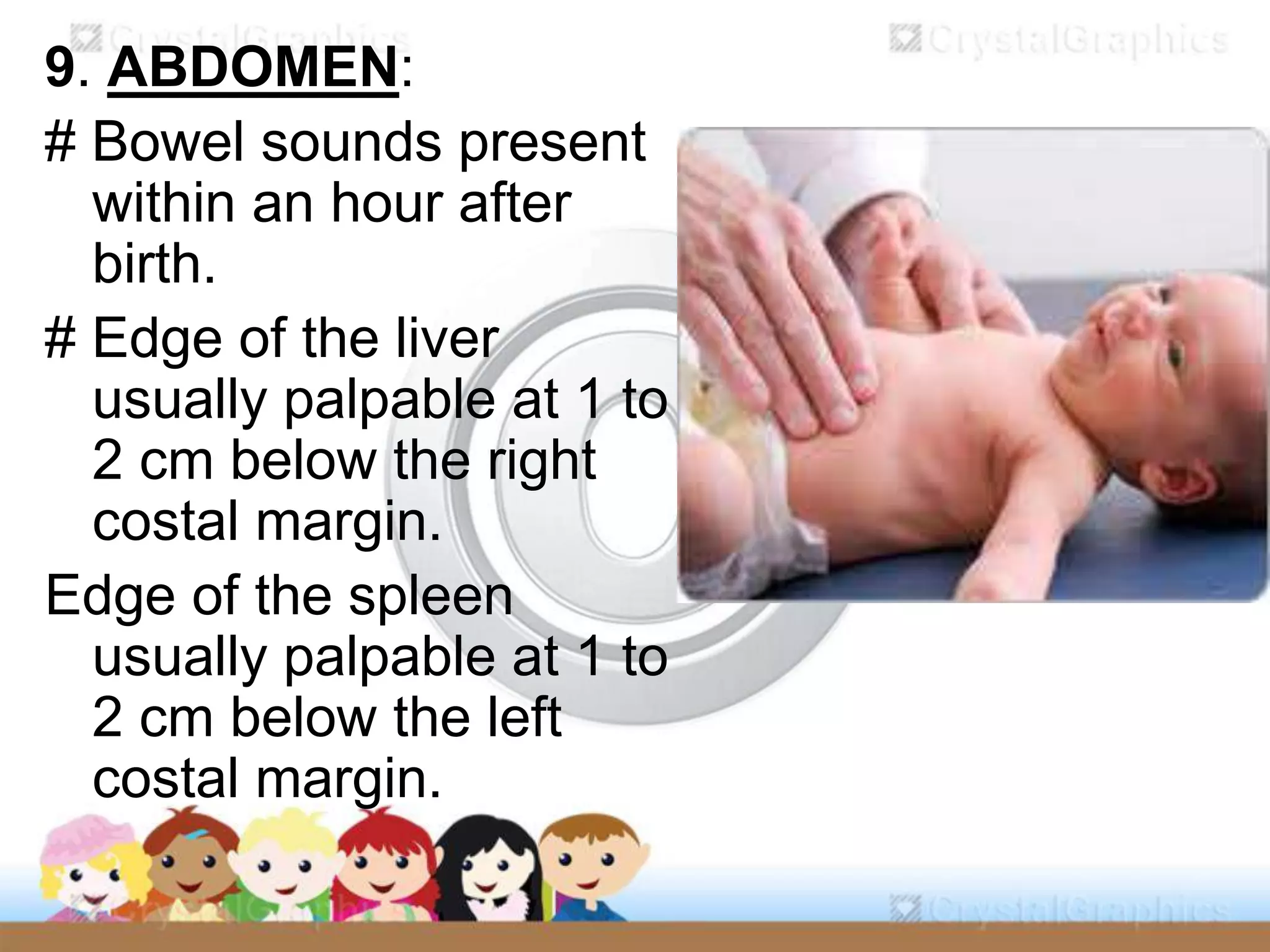
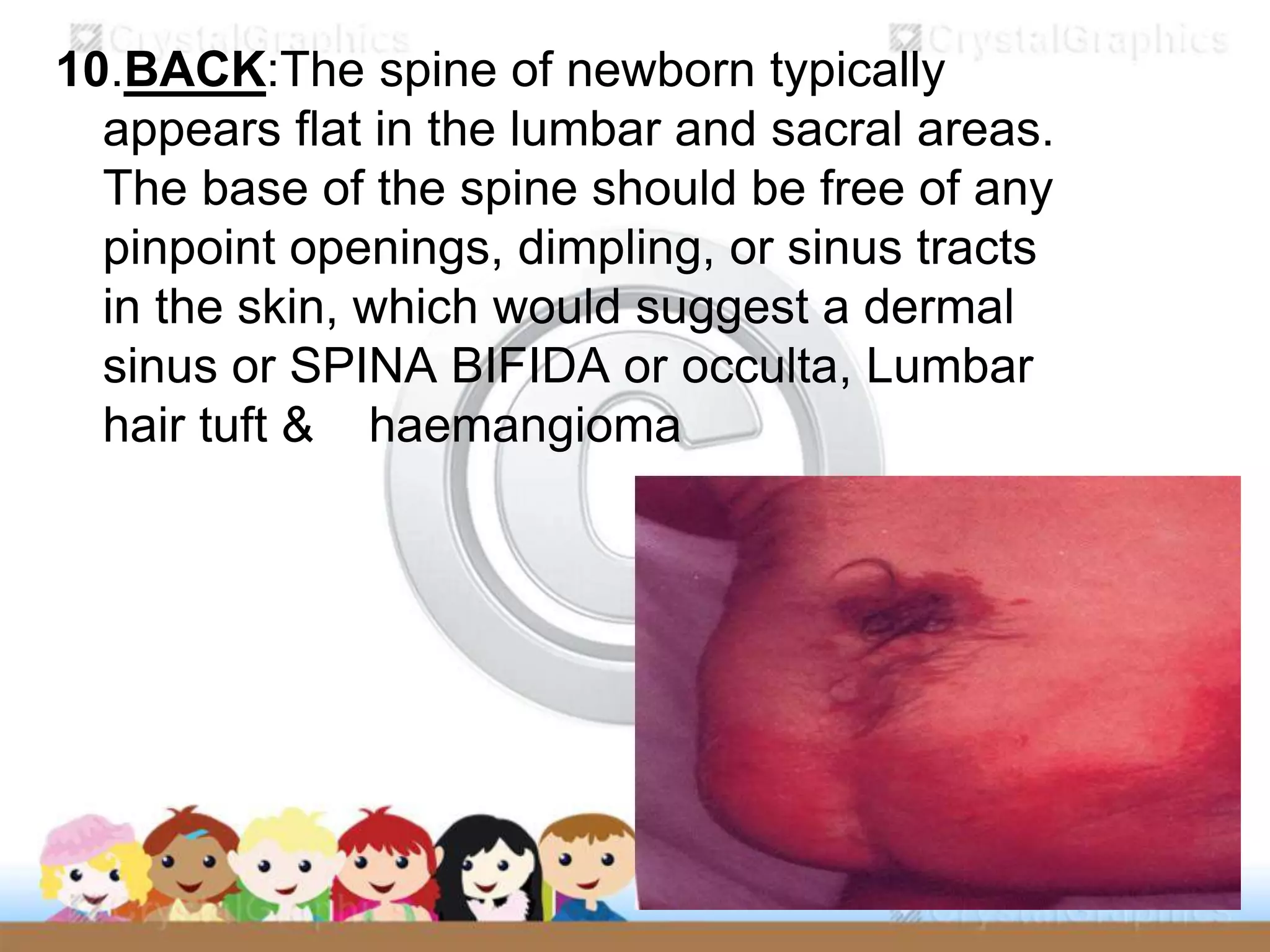
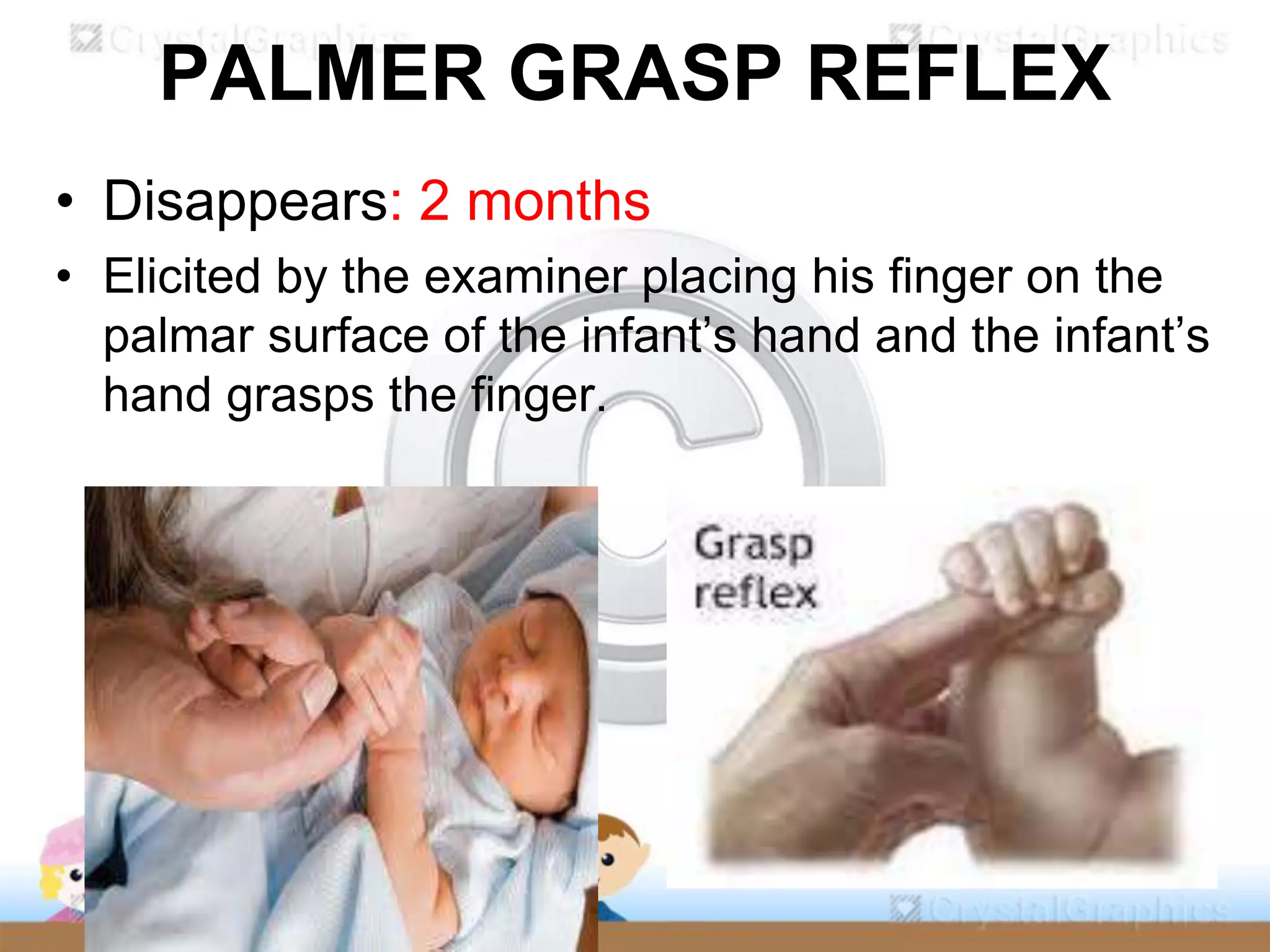
The document outlines the systematic examination of newborns, focusing on their physical and neurological assessment immediately after birth and during follow-up visits. Key objectives include evaluating the infant's health, identifying abnormalities, and monitoring development, alongside procedures and terminologies related to gestational age and vital signs. It specifies various aspects of the physical examination, such as measurements, skin characteristics, reflexes, and anatomical checks, along with implications for potential health issues.