DEFINITION
A healthy infantborn at term b/w 38-42 wks should
have average birth wt, cries immediately following
birth, establishes independent rhythmic respiration &
quickly adapts to the changed envt.
3.
HISToRY
MATERNAL HISTORY
Age, parity, medical disorders, menstrual history
PREGNANCY PROBLEMS
Present & past, drugs, IUFD, pre-eclampsia, IUGR,
prematurity.
LABOUR & DELIVERY HISTORY
Duration, anaesthesia.
4.
Physiology of thenewborn
(1) Temperature control
Heat production ;
basal metabolism, Shivering, chemical thermogensis
Heat loss ;
radiation, evaporation, convection, conduction
Neonate ;
subcut.fat tissue, body surface area, amniotic fluid
Neutral thermal environment
Infant heat regulation mechanism has not fully
developed. His temp rapidly reflect to the envt..
5.
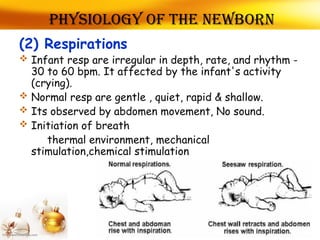
(2) Respirations
Infantresp are irregular in depth, rate, and rhythm -
30 to 60 bpm. It affected by the infant's activity
(crying).
Normal resp are gentle , quiet, rapid & shallow.
Its observed by abdomen movement, No sound.
Initiation of breath
thermal environment, mechanical
stimulation,chemical stimulation
Physiology of the newborn
6.
(3) Blood Pressure
The average blood pressure is 72/42. (45-60/25-
40)mmhg.
A drop in systolic BP of about 15 mm Hg the 1st
hour
after birth is common.
The newborn's BP may be taken with a Doppler blood
pressure device.
This greatly improves accuracy.
Physiology of the newborn
7.
(4) Pulse
Thenormal pulse is 120 to 140 (bpm).
The rate may rise to 160 bpm when the infant
is crying
It drop to 100 bpm when the infant is
sleeping.
The apical pulse is considered the most
accurate
Physiology of the newborn
8.
Physiology of NEWBORN
INFANT'SHEAD
The newborn infant's head represents
one-fourth of his total body length. Its
circumference is equal to that of his
abdomen or chest. The average size is
13" to 14" inch (33-35 cm). The head is
shaped or molded as it is forced through
the birth canal in vertex presentations.
9.
Molding
During delivery,for the large head to pass
through the small birth canal, the skull bones
may actually overlap in a process referred to
as molding. -disappears a few hours after
birth.
10.
Fontanels
The infant'sskull is separated into six bones
one from another along the suture lines
Where more than two bones come together,
the space is called a fontanel.
This is the unossified space or soft spot
between the cranial bones of the skull in an
infant. The infant's pulse is sometimes visible
there.
The anterior fontanel
Its is located at the intersection of the
sutures of the two parietal bones and the
frontal bones.
It is diamond-shaped and strongly pulsatile.
It normally closes at 9 to 18 months of age.
13.
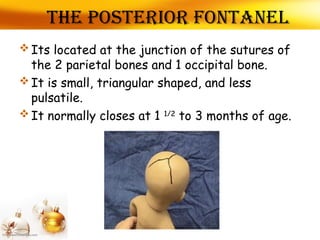
The posterior fontanel
Its located at the junction of the sutures of
the 2 parietal bones and 1 occipital bone.
It is small, triangular shaped, and less
pulsatile.
It normally closes at 1 1/2
to 3 months of age.
14.
Fontanels
Large fontanels:
-Hypothyroidism, chromosomalabnormalities
Bulging fontanels:
-Increased ICP, Meningitis, Hydrocephalus
Decreased fontanels:
-Dehydration
Small fontanels:
-Hyperthyroidism, microcephaly, craniosyntosis
Increased ICP:
- Bulging ,separation of suture lines, prominent veins of the
scalp
15.
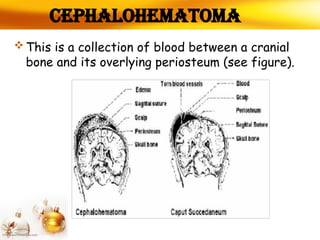
Cephalohematoma
This isa collection of blood between a cranial
bone and its overlying periosteum (see figure).
16.
Cephalohematoma cont….
Causedby pressure of the fetal head against
the maternal pelvis-labour
It varies in size
firm to the touch and tends to increase in size
from 1 to 3 days
then become softer and more fluctuant
17.
Caput Succedaneum
Itsabnormal collection of fluid under the
scalp on top of the skull that may or may not
cross the suture lines, depending on size.
Pressure on the presenting part of the fetal
head against the cervix during labor may
cause edema. This will be absorbed within 2 or
3 days.
18.
NEWBORN INFANT'S EYESAND EARS
EYES :
• (1) Color: At birth, the iris color is usually
grayish-blue or brown in dark.
• A gradual deposition of pigment produces the
final eye color -3 to 6 months or one year
19.
EYES cont…..
• (2)Pupils: The pupils do react to light
• (3) Lacrimal apparatus : is small and
nonfunctioning at birth until 1 to 3 months of
age.
• (4)Examined for :
A) congenital cataract ,
20.
B) Brash fieldsspots : in the iris small white or
grayish/brown spots -Down syndrome
C) Sub conjunctival haemorrhage
21.
Ears
Ears tobe folded and creased. A line drawn
through the inner and outer canthi of the eye
should come to the top notch of the ear
where it joins the scalp (see figure )-responds
to sound at birth.
Vernix Caseosa
• Thisis a soft, white, cheesy, yellowish cream
on the infant's skin at birth (see figure). It is
caused by the secretions of the sebaceous
glands of the skin
26.
• These aretiny sebaceous retention cysts. They
appear as small white or yellow dots and are
common on the nose, forehead, and cheeks of the
infant. Its pin head size and opalescent. Its is
due to blocked sweat and oil glands -disappear a
few weeks.
MILLIA
27.
Mongolian spot
• Theseare blue-black colorations on the
infant's lower back, buttocks, and anterior
trunk. It disappear in early childhood.
28.
• it isa benign self involuting tumor of endothelial
cells (the cells that line blood vessels). -appears
during the 1ST
days or wks of life and will have
resolved at the latest by age 10. It is the most
common tumor.
Hemangioma
Erythema toxicum
• Arash is a change in the color or
texture of the skin. A skin rash can be
flat, bumpy, scaly, red, skin-colored, or
slightly lighter or darker than skin color.
31.
Vellous hair
• Velloushairs are short, fine, light colored,
and barely noticed, as compared with terminal
hair.Vellus hair is usually less than 2 mm long
and the follicles are not connected to
sebaceous glands
32.
Physiology of thenewborn skin (cont…..)
JAUNDICE:
yellow discoloration
PALLOR:
due to anaemia, asphyxia, shock, edema
PETECHIAE:
small, blue-red dots on the infants-grain
PLETHORA:
seen in polycythemia infants
STROKE BITES:
present small reddened areas on eyelids, mild
forehead, nape of the neck
HEMANGIOMA:
strawberry mark, characterised by a dark or bright
red raised, rough surface
33.
(6) Digestive
Bowelmusculature ; weak
Mouth
Stomach: capacity - 1 to 2 ounces (30 to 60 ml) at
birth
- digestion of simple CHO, proteins, limit fat
digestion
Meconium passage ; 10hr after birth
> 24hr
The first stools after birth and for three to four
days afterwards are called meconium.
Transitional stool ; the first 4ds-2wk
Physiology of the newborn
34.
CHARACTERISTICS OF THENEWBORN
CIRCULATORY SYSTEM
• Blood Coagulation: the first few days of life, the
prothrombin level decreases and clotting time in
all infants is prolonged. This process is most acute
b/w the 2nd
& 5th
PN days
• Blood Flow: umbilical blood stops flowing at birth,
sudden pressure differences occur within the
circulatory system. These differences cause the
blood flowing to the lungs and liver to increase
and the blood flowing through the bypass channels
to decrease.
35.
(7) ENDOCRINE SYSTEM
Vaginal discharge and/ blding : may occur in
female infants. This discharge is white mucoid
in color. The entire process terminates in one
to two days.
Enlargement of the mammary glands : may
occur in both sexes. This is particularly
noticeable about the 3 day of life. Breast
secretion may also occur. Swelling usually
subsides in 2 to3weeks.
Physiology of the newborn
36.
(8) Urinary system
Immature nephron 106
GFR ; 25% of adult value
Low tubular concentration function
Urination ; the 1st
day 15ml
10th day 100-300ml
Urinary sys. work-up ; after 2days
Urate excretion
Physiology of the newborn
Asymmetric tonic neckreflex
The infant assumes a fencer's position. His
arm and leg on one side is extended, the opposite
side is flexed. His head is turned toward
extended side.
neurological development is
depenton GESTATIONAL AGE
Charecter ≤36 Weeks 37-28 Weeks ≥ 39 Weeks
Sole creases 1-2 transferse
creases: post ¾ sole
smooth
Multiple creases,
Anterior 2/3 of heel
smooth
Entire sole
covered with
creases
Breast Nodule 2mm 4mm 7mm
Scalp hair Fine Fine Coarse, silky
Ear lobe No cartilage Moderate Stiff ear lope,
thick cartilage
Testes and
Scrotum
Testes partially
descended scrotum
small and few rugae
- Testes fully
descended
scrotum – normal
size prominent
rugae
45.
Hematology
Blood vol.- 85ml/kg
Hb% - 19.3 g/dl(18-20)gm%
WBC - 9000-30000/mm3
Platelets - nl – prolongation (the first2-3ds)
Metabolic acidosis
RBC – 6 to 8 million/cumm
platelets – 3,50,000/cumm
Sedimentation rate – markedly elevated
Clotting power poor – b/c Deficient of vit-k
Physiology of the newborn
Physical examination
of thenewborn
• Initial exam ;
– every 30min after birth or until stabilized
• Second exam ;
– within 24hr of birth
48.
Physical examination(1)
• Vitalsign
• weight, length, head circumference
• Gestational age
• General appearance
state of consciousness
muscle tone
activity
obvious anomalies/injuries
49.
Physical examination(2)
• Skintexture of skin
vernix
lanugo
milia
erythema toxicum
hemangioma/nevi
dermal sinus
jaundice
-smooth, flexible, good skin, warm,
turgor
Apgar score
sign 01 2
Heart rate absent Below 100 Over 100
Resp.effort absent Slow,irregular Good crying
Muscle tone limp Some flexion Active motion
Response
to catheter in
nostril
No response grimace Cough/sneeze
color Blue, pale Body pink,
ext.blue
Complete pink
65.
CHANGES DURING THE1ST
WEEK
• POSITION:
– the feet are less dorsiflexed ,
– Hands are less elenched.
• WT:
– 4th
& 5th
day-10% loss,
– 25-30 gm /day
• SKIN:
– pinkish to pale
– Become dry & scaly
– Slight yellow-60% baby
• HEAD:
– Moulding& caput- disappear
• TEMPRATURE : Varition occur
• ABDOMEN:
• Cord – dry, falls-5th
-7th
day
66.
• STOOL:
• Meconiun:
– 3-4times, 2-3 days-12 hrs
– 3rd
-4th
day –changing stool –yellowish brown
– Bottle feeding-hard , pale in colour
– No of stool passed- 2-3 times /24 hrs
• URINE:
– DURING 1ST
WEEK-60ml/24 hrs
– U/O increase to 200-300 ml/day by the 7th
day
CHANGES DURING THE 1ST WEEK