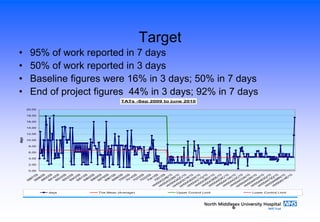
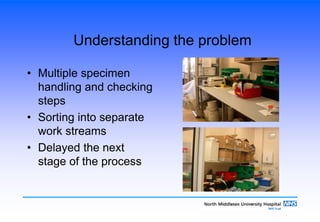
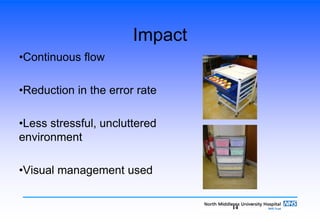
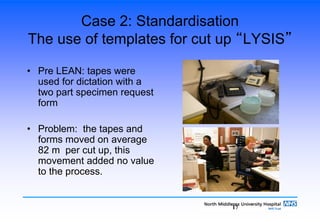
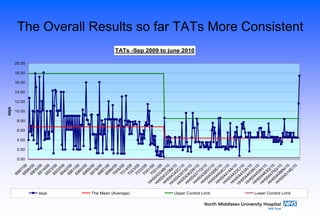
The document summarizes lean process improvements implemented in a histopathology department. Broad aims were to share lean solutions, debate strengths/weaknesses, and network. The presentation describes implementing standardized work templates to reduce movement and errors, optimizing layout to reduce travel distance, and introducing a pull system for consultant reporting to better match workload to availability. Measurable outcomes included a 43% reduction in specimen checks, 92% of work reported within 7 days (up from 50%), and decreased consultant reporting time from 4.5 to 1.8 days.