Downloaded 18 times
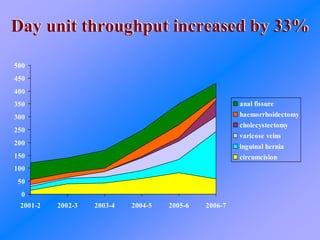

The document discusses using lean principles and value stream mapping to improve operating theatre utilization and patient flow at a hospital. It describes identifying high-volume procedures, standardizing equipment and scheduling for these "green stream" cases, and coordinating staff to allow continuous workflow. As a result, day unit throughput increased 33%, inpatient beds were reduced, and staff communicated better with fewer delays. Lessons included needing committed teams and measuring utilization continuously.

















































![Delivering care in efficient environment medicall 2011 [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/deliveringcareinefficientenvironment-medicall2011compatibilitymode-110831063224-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![MS Project Management presentation%20 Nhs%20 Rotherham[1]](https://cdn.slidesharecdn.com/ss_thumbnails/project20management20presentation20nhs20rotherham1-13324406433982-phpapp02-120322132605-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)













































