Downloaded 76 times

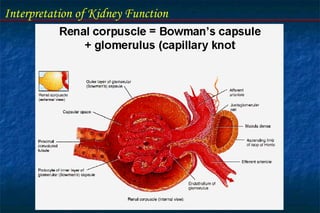
![Interpretation of Kidney Function
Renal Functions : Acid-Base balance
Stabilizes blood pH (in company
with buffer systems and regulation
of [CO2]
Regulates loss of H+ ions (acid)
Regulates loss of HCO-3 ions
(base)
Normal plasma pH
7.35-7.45
Acidosis
pH < 7.35
Alkalosis
pH > 7.45](https://image.slidesharecdn.com/kidneyfunctiontestsbymoustafarizk-171011065403/85/Kidney-function-tests-by-moustafa-rizk-21-320.jpg)
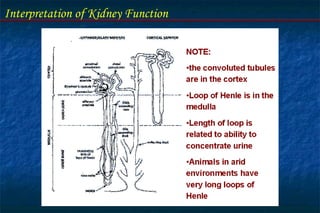
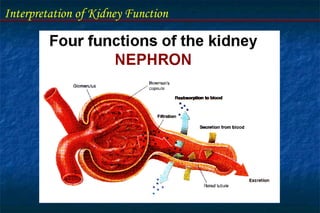
![Interpretation of Kidney Function
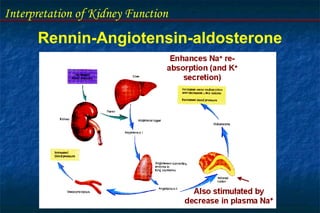
Regulates plasma concentrations of electrolytes
(e.g. Na+
, K+
, Cl-
, and other ions)
Water retained or lost in response to plasma osmolality
(normal plasma osmolality 290 mOsm/kg H2O).
ADH mechanism
Controls loss in urine
Contributes to plasma [Ca2+] regulator by vitamin D
(calcitriol) regulation
Renal activation of calcitriol increases Ca2+
uptake
from gut.](https://image.slidesharecdn.com/kidneyfunctiontestsbymoustafarizk-171011065403/85/Kidney-function-tests-by-moustafa-rizk-22-320.jpg)
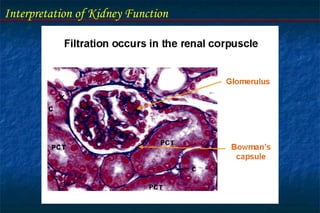
![3-Urinary acidification test:
[H+
] of urine is normally > [H+
] of blood & of GF.
In order to achieve this degree of acidification, the Kidney:
- Reabsorbs [HCO3-
].
- Excretes [H+
] partly as free [H+
] and partly as NH4
Salt or in combination with anions principally inorg Ph.](https://image.slidesharecdn.com/kidneyfunctiontestsbymoustafarizk-171011065403/85/Kidney-function-tests-by-moustafa-rizk-55-320.jpg)


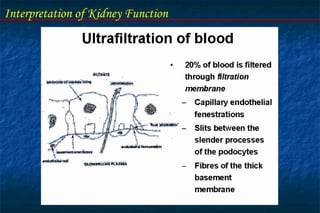
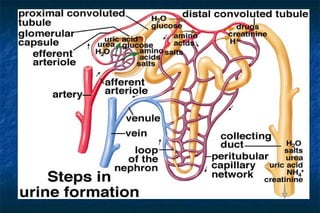
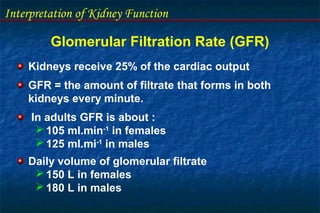
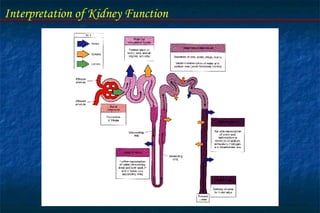
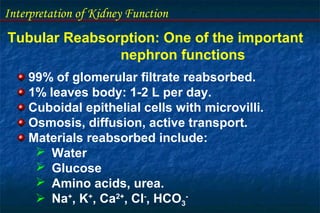
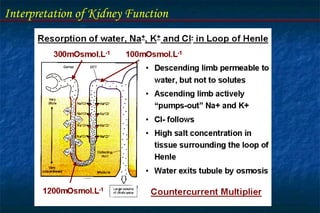
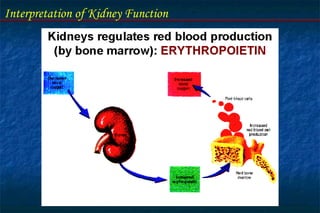
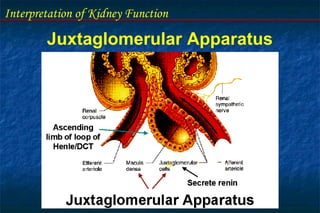
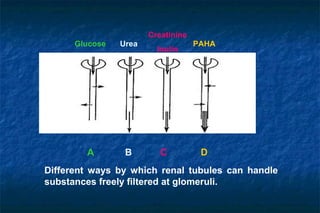
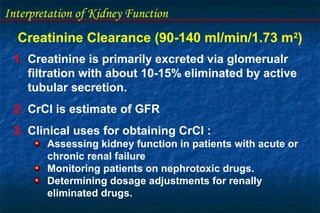
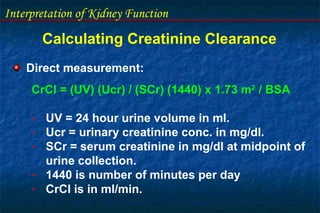
The document discusses the interpretation of kidney function through laboratory tests. It describes the physiologic role and functional units of the kidney. Key points include: - The nephron is the functional unit of the kidney, which filters blood to form urine and regulates electrolytes and acid-base balance. - Glomerular filtration rate (GFR) and creatinine clearance are tests used to assess kidney filtration function. Creatinine clearance is estimated based on creatinine levels in serum and urine. - Tubular function tests include urine concentration and acidification to evaluate the kidney's reabsorption and regulatory roles. Assessing these functions provides insight into renal disorders.























































































