Downloaded 313 times
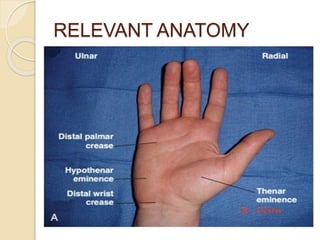

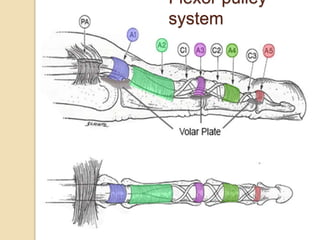
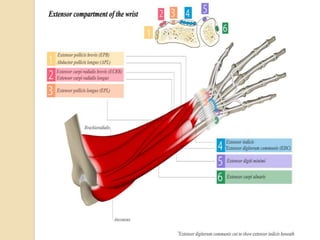
















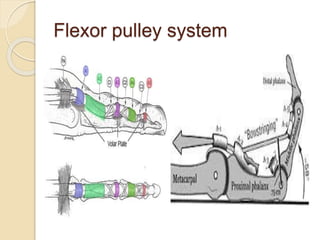
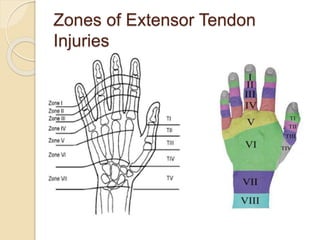
















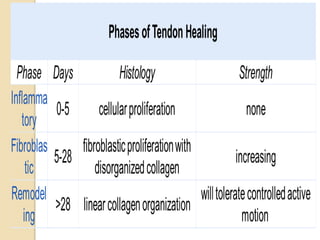









The document discusses hand injuries and their management. It covers relevant hand anatomy, types of common hand injuries including tendon injuries, fractures, and dislocations. The key principles of management are early debridement and stabilization of injuries, restoration of anatomy, and rapid mobilization. Specific techniques are described for repairing tendons, fixing fractures like Bennett's fracture, and achieving proper skeletal stabilization while preserving hand function.



































































