





















![Volatile sulphur compounds → hydrogensulphide [H2S,
rotten egg smell], dimethyl sulphide [(CH3)2S, rotten
cabbage smell, and methyl mercaptan [CH3SH, fecal smell].
Non - sulphur containing substances → diamines
[cadaverine (cadaver smell) and putrescine (rotten meat
smell), acetone and acetaldehyde
ETIOLOGY
Yaegaki K, Sanada K. Volatile sulphur compounds in mouth air from clinically healthy
subjects and patients with periodontal disease. J Periodontol Res 1992;27:233-8.](https://image.slidesharecdn.com/jc12halitosis-160711133412/85/Halitosis-Dr-Sanjana-Ravindra-31-320.jpg)















































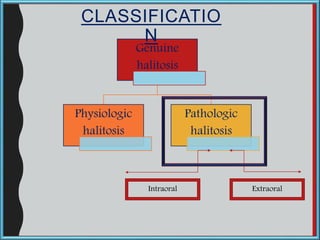
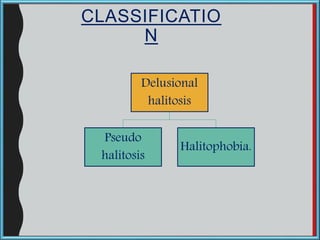
The document discusses halitosis, defined as the unpleasant odor emanating from the breath, which can originate from both oral and non-oral sources. It covers the etiology, diagnosis, and management of halitosis, highlighting its multifactorial causes, including oral hygiene, medical conditions, and psychological aspects. Moreover, the text provides historical context, epidemiological data, classifications, and diagnostic methods for managing this condition.




































































































