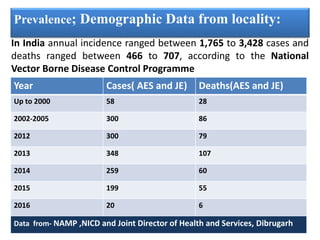
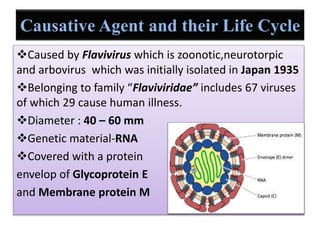
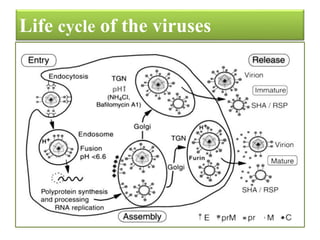
This document summarizes a study on Japanese encephalitis (JE). It begins with an introduction to JE, describing its discovery in 1871 in Japan and transmission via Culex mosquitoes. Symptoms and prevalence data from India and the locality are discussed. The causal virus is described along with its life cycle. Diagnosis methods like ELISA, PRNT and RT-PCR are covered. Preventive measures like vaccination campaigns and vector control are summarized. Conclusions note the role of environmental factors and need for improved immunization programs to control the disease.