CM 8.1
Describe anddiscuss the
epidemiological and
control measures
including the use of
essential laboratory tests
at primary care level for
communicable disease
(Japanese Encephalitis)
Dr.Parimita
Roychoudhury
Assistant Professor,
DMCH, Dhubri
2.
LEARNING OBJECTIVES
• Atthe end of the session students will be able to
1.Define and differentiate between Acute Encephalitis syndrome and
Japanese Encephalitis
2.Enumerate and Describe the epidemiological triad of Japanese
Encephalitis
3.Describe the clinical features and differential diagnosis of Japanese
Encephalitis
4.Describe the Laboratory diagnosis
5.Describe the Prevention and control methods of Japanese Encephalitis
3.
Vector- living organismthat transmits an infectious agent from
an infected animal to a human or another animal
a) Invertebrate type : Arthropod vector fall
into 7 categories.
(1) Diptera - flies and mosquitoes
(2) Siphonaptera - fleas
(3) Orthoptera - cockroaches
(4) Anoplura - sucking lice
(5) Hemiptera - bugs, including kissing bugs
(6) Acarina - ticks and mites
(7) Copepoda - cyclops
b) Vertebrate type
— Mice, rodents,
bats.
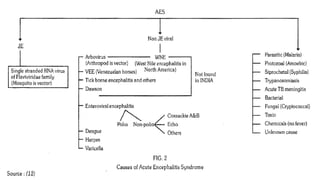
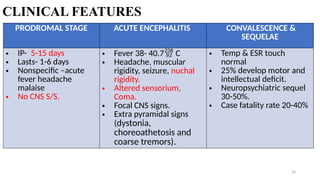
AES
• Any personof any age who develops
acute onset of fever & change in
mental status (confusion,
disorientation, coma, inability to talk,
new onset seizure- excluding simple
febrile seizure).
• Cause- virus, bacteria, fungus,
parasites, spirochetes, chemical/ toxins.
• Group of diseases having similar S/S.
JE
• Common cause of AES.
• A PATIENT WILL COME WITH S/S OF AES
NOT JE.
INTRODUCTION
8
•JE is azoonotic disease transmitted by mosquito
•Case-fatality rate among those with encephalitis can be as
high as 30%
•24 countries in the WHO South-East Asia and Western
Pacific regions have endemic JEV transmission
•There is no cure for the disease
9.
History of JE
•1870-Japan “Summer Encephalitis” epidemic
• 1924-Great epidemic in Japan ,case fatality 62%
• 1940 to 1954-Epidemic in China,Korea,India
• 1983-Immunization in human first started in Korea
• 2006 –JE vaccine introduced after campaign in endemic districts in
India
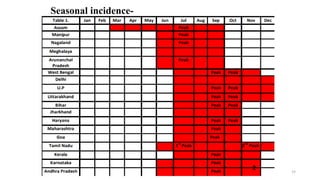
•The disease isendemic in 21 states.
Assam, Bihar, Haryana. Uttar
Pradesh, Karnataka, West Bengal
and Tamil Nadu report out-breaks
every year and contribute about 80
per cent of cases and deaths
12.
ASSAM HISTORY
• 1963-Serologicalevidence
• 1976- First epidemic in Upper Assam
• 1978- Virus isolation from Brain tissue at AMCH
• 1978, 1982, 1986 -Greater magnitude epidemic.
Most affected districts are Dibrugarh, Dhemaji,
Lakhimpur, Sivasagar, Jorhat, Golaghat, Tinsukia &
Sonitpur.
12
13.
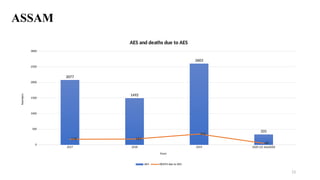
ASSAM
13
2017 2018 20192020 (23 July2020)
0
500
1000
1500
2000
2500
3000
2077
1492
2603
331
178 183
345
48
AES and deaths due to AES
AES DEATH due to AES
Years
Numbers
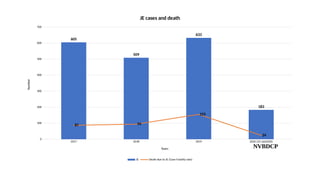
14.
2017 2018 20192020 (23 July2020)
0
100
200
300
400
500
600
700
605
509
633
183
87 94
155
24
JE cases and death
JE Death due to JE (Case Fatality rate)
Years
Number
NVBDCP
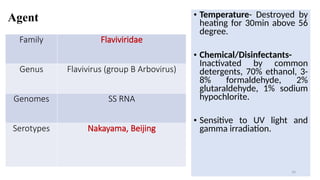
Agent
Family Flaviviridae
Genus Flavivirus(group B Arbovirus)
Genomes SS RNA
Serotypes Nakayama, Beijing
• Temperature- Destroyed by
heating for 30min above 56
degree.
• Chemical/Disinfectants-
Inactivated by common
detergents, 70% ethanol, 3-
8% formaldehyde, 2%
glutaraldehyde, 1% sodium
hypochlorite.
• Sensitive to UV light and
gamma irradiation.
16
17.
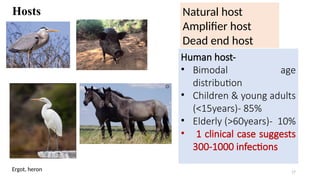
Hosts
17
Human host-
• Bimodalage
distribution
• Children & young adults
(<15years)- 85%
• Elderly (>60years)- 10%
• 1 clinical case suggests
300-1000 infections
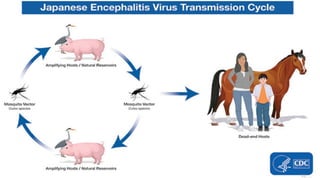
Natural host
Amplifier host
Dead end host
Ergot, heron
18.
Enviroment
• Temperate- Latesummer/early autumn
Tropical- Year round
• Endemic in temperate & tropical regions of
Asia.
• Epidemics- Paddy season (monsoon & post
monsoon)
• Primarily rural areas. It has spread to new areas
d/t agricultural development supported by
irrigation programme
18
Vector
20
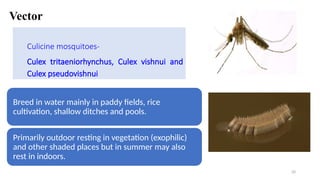
Culicine mosquitoes-
Culex tritaeniorhynchus,Culex vishnui and
Culex pseudovishnui
Breed in water mainly in paddy fields, rice
cultivation, shallow ditches and pools.
Primarily outdoor resting in vegetation (exophilic)
and other shaded places but in summer may also
rest in indoors.
• Human tohuman transmission has not so far been
recorded Man is an incidental dead-end host
• Cattle and buffaloes may also be infected with the JE
virus; although they may not be natural hosts of JE
virus, they act as "mosquito attractants”
• 9-12 days incubation period, they can transmit the
virus to other hosts
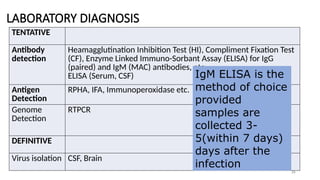
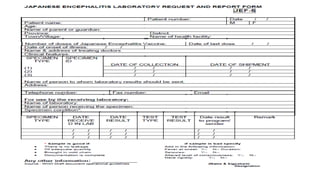
LABORATORY DIAGNOSIS
26
TENTATIVE
Antibody
detection
Heamagglutination InhibitionTest (HI), Compliment Fixation Test
(CF), Enzyme Linked Immuno-Sorbant Assay (ELISA) for IgG
(paired) and IgM (MAC) antibodies, etc.
ELISA (Serum, CSF)
Antigen
Detection
RPHA, IFA, Immunoperoxidase etc.
Genome
Detection
RTPCR
DEFINITIVE
Virus isolation CSF, Brain
IgM ELISA is the
method of choice
provided
samples are
collected 3-
5(within 7 days)
days after the
infection
27.
27
Specimen collection-
• 4days after onset for
isolation.
• 5 days after onset for IgM
ab.
Laboratories-
• District sentinel
surveillance laboratories
• National laboratories/
Referral laboratories
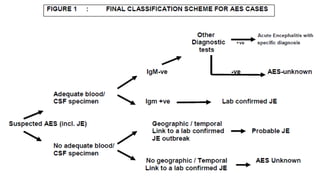
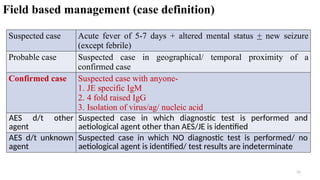
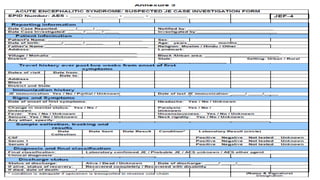
Field based management(case definition)
31
Suspected case Acute fever of 5-7 days + altered mental status + new seizure
(except febrile)
Probable case Suspected case in geographical/ temporal proximity of a
confirmed case
Confirmed case Suspected case with anyone-
1. JE specific IgM
2. 4 fold raised IgG
3. Isolation of virus/ag/ nucleic acid
AES d/t other
agent
Suspected case in which diagnostic test is performed and
aetiological agent other than AES/JE is identified
AES d/t unknown
agent
Suspected case in which NO diagnostic test is performed/ no
aetiological agent is identified/ test results are indeterminate
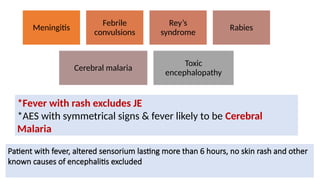
WHAT HAVE WELEARNT TILL NOW………
• Viral infection
• Fever
• +Altered sensorium
HOW DO WE START MANAGEMENT-
• History
• Clinical examination (General & Systemic)
34.
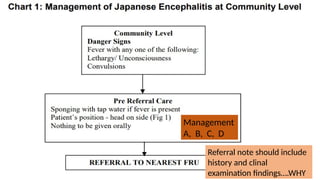
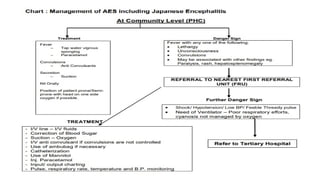
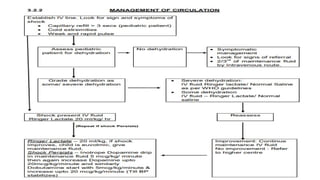
MANAGEMENT OF CASES
•Symptomatic and supportive
• Refer to nearest FRU if anyone develops- Lethargy,
Convulsions, Unconsciousness
• Refer to higher center directly if develops- Shock,
Needs ventilator, Unmanageable cyanosis.
• Suspected case referred should be confirmed with 2
diagnostic test-
1. RT-PCR
2. Detection of- virus ag/ genome.
34
35.
Management
A, B, C,D
Referral note should include
history and clinal
examination findings….WHY
37.
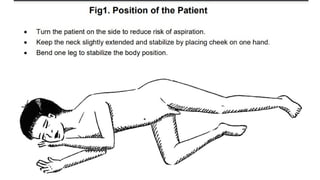
The treatment ofthe patients may require as follow:-
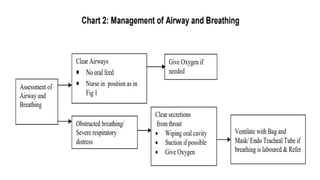
1.) Management of Airways and Breathing.
2.) Management of Circulation.
3.) Control of Convulsion and Intracranial pressure
4.) Control of Temperature
5.) Fluid and Electrolytes and Calories/ Nutrition
6.) General management
7.) Specific treatment of any for treatable cause
8.) Investigations, Sample Collection & Transportation
9.) Reporting of a case
10.) Rehabilitation.
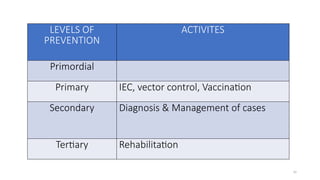
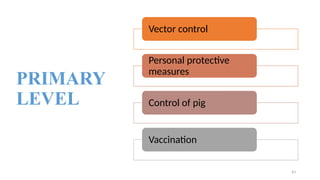
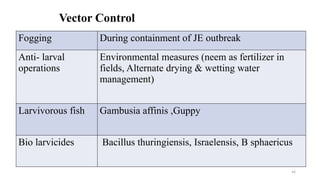
Vector Control
Fogging Duringcontainment of JE outbreak
Anti- larval
operations
Environmental measures (neem as fertilizer in
fields, Alternate drying & wetting water
management)
Larvivorous fish Gambusia affinis ,Guppy
Bio larvicides Bacillus thuringiensis, Israelensis, B sphaericus
44
45.
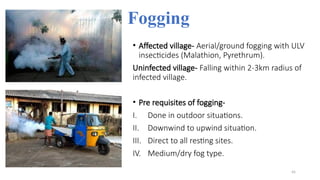
Fogging
• Affected village-Aerial/ground fogging with ULV
insecticides (Malathion, Pyrethrum).
Uninfected village- Falling within 2-3km radius of
infected village.
• Pre requisites of fogging-
I. Done in outdoor situations.
II. Downwind to upwind situation.
III. Direct to all resting sites.
IV. Medium/dry fog type.
45
Control of Pig
•Immunization- Inactivated/ attenuated vaccines.
• Challenge- difficult to ensure complete coverage due to
rapid breeding & limited vaccine effectiveness.
• Slaughtering of pig
• Mosquito proof piggeries
• Segregating pigs 4-5km away from human habitations
48
49.
Vaccination in human
•3 types of vaccines-
1. Inactivated brain derived and purified type- Nakayama/ Beijing strain
2. Cell culture derived- Inactivated- Beijing P-3 strain,Kolar 821564XY
3. Cell culture derived- Live attenuated- SA 14-14-2 strain
• Recommended for- Children, Laboratory staff, Travellers (Visiting >30days)
• Dose & Schedule-
0.5ml for <3years, 1ml for >3years.
2 dose 1 month apart
Booster- 1year, every 3rd
year till 15 years
49
• Periodicity ofReports-
I. Daily report- Outbreak situation
II. Weekly report- Transmission period
III. Monthly report- Inter-epidemic period.
• Forms-
I. AESF 1/1A- From states
II. AESF 2/2A- Districts
III. AESF 3- Line listing form
IV. AESF 4- Case investigation form
53
56.
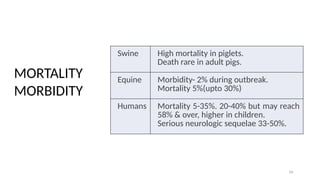
MORTALITY/
MORBIDITY
56
Swine High mortalityin piglets.
Death rare in adult pigs.
Equine Morbidity- 2% during outbreak.
Mortality 5%(upto 30%)
Humans Mortality 5-35%. 20-40% but may reach
58% & over, higher in children.
Serious neurologic sequelae 33-50%.
MORTALITY
MORBIDITY









































![UG QUIZ [Autosaved].pptxjkoopookkklllppp](https://cdn.slidesharecdn.com/ss_thumbnails/ugquizautosaved-250807170324-b21c6806-thumbnail.jpg?width=640&height=640&fit=bounds)




















