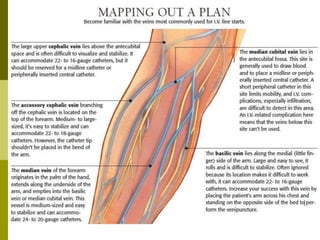
This document provides information about intravenous (IV) therapy, including statistics on its use, common complications, prevention strategies, and proper procedures. It notes that 85% of hospitalized patients receive IV therapy. Common complications include phlebitis (vein inflammation), infiltration of non-vesicant fluids into surrounding tissues, extravasation of certain drugs into tissues, and infection. Proper insertion technique and site care can help prevent complications.