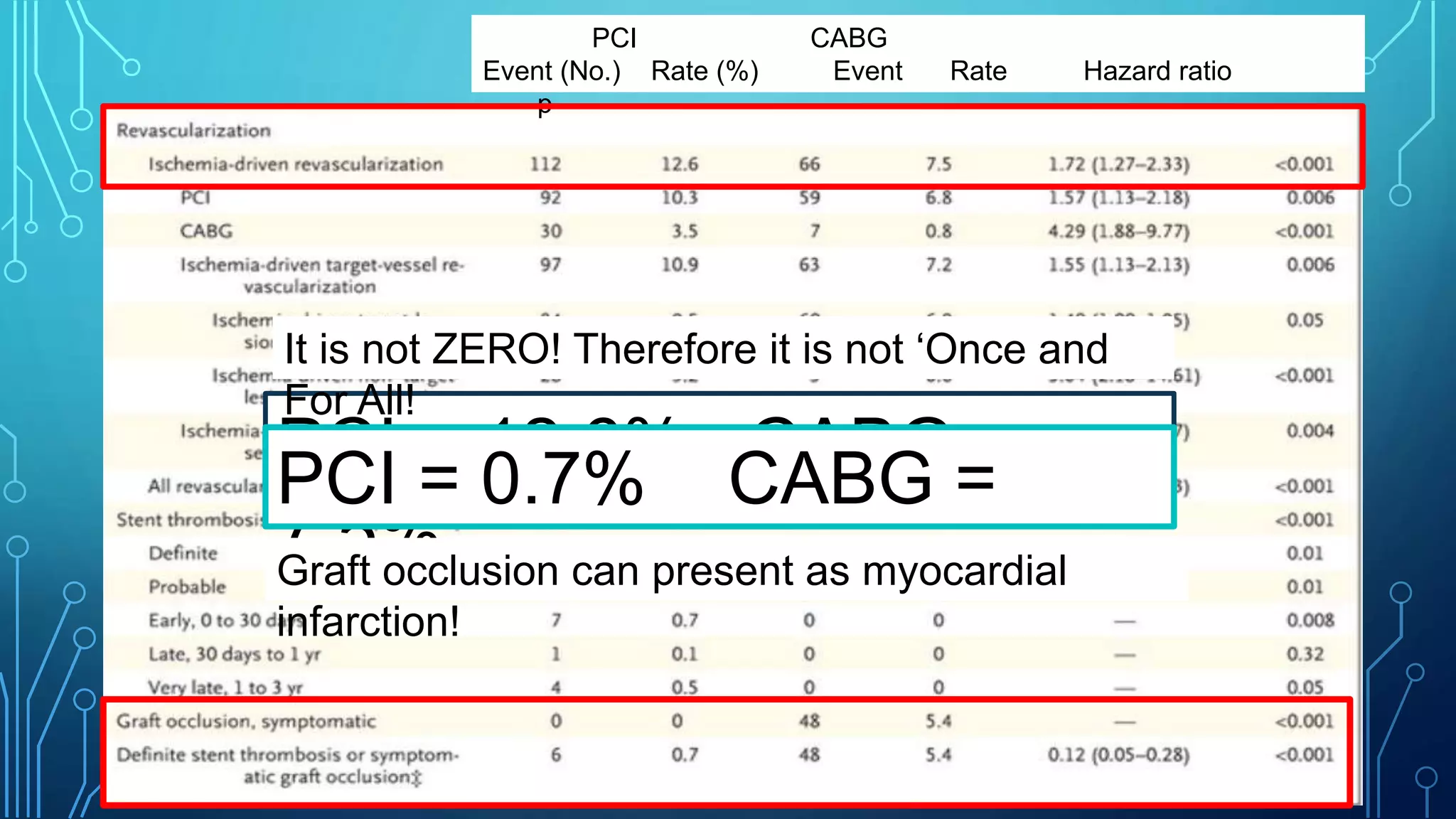
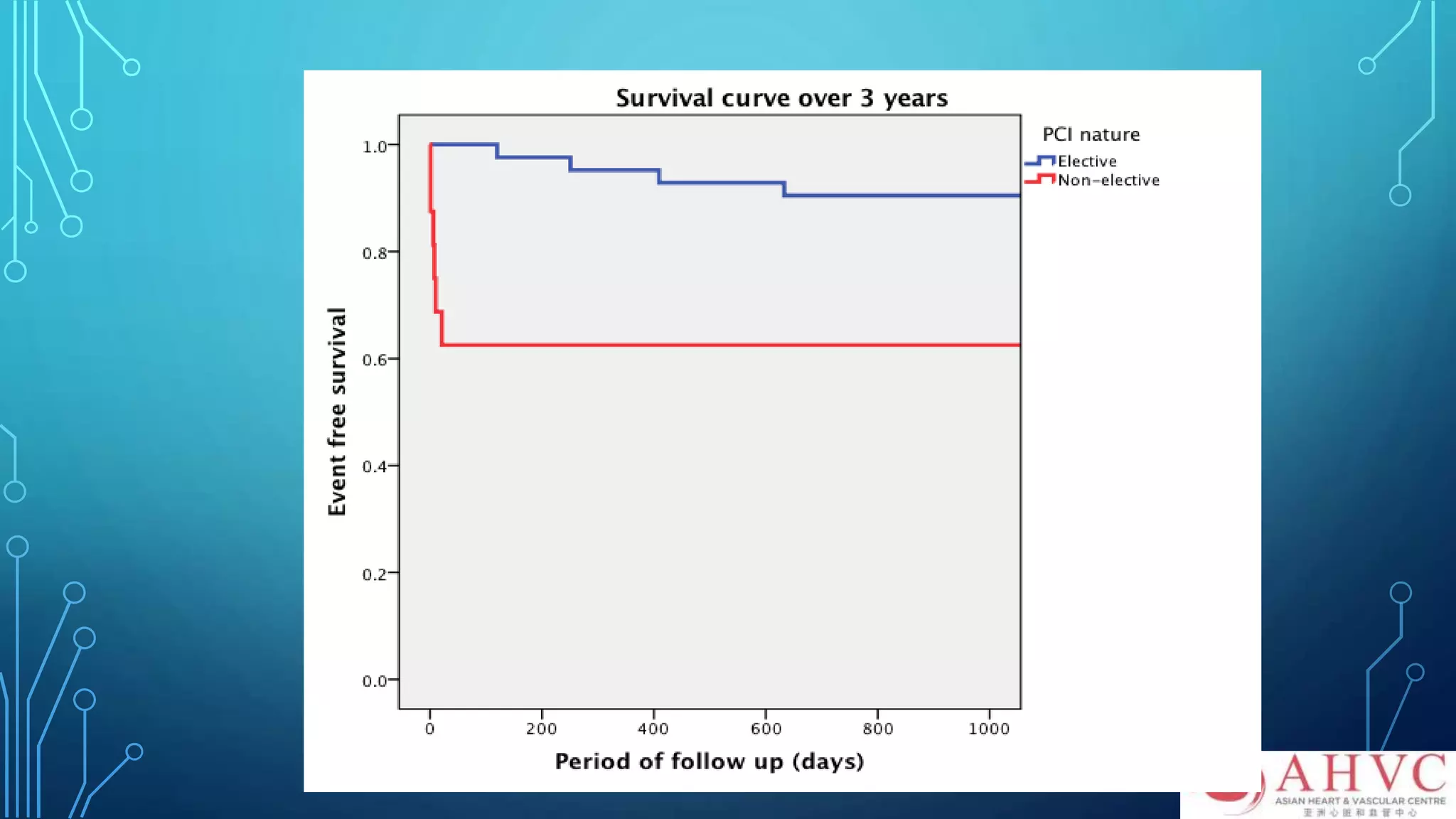
This document discusses the management of unprotected left main disease and chronic total occlusions (CTOs) in coronary artery disease, highlighting the evolving guidelines and the effectiveness of percutaneous coronary intervention (PCI) compared to coronary artery bypass grafting (CABG). It emphasizes that while CABG has traditionally been viewed as the superior option, data show that PCI can also be a viable alternative when performed by experienced operators. The document presents a detailed analysis of procedural outcomes for both approaches and advocates for the treatment of CTOs, stressing the importance of skilled interventional cardiologists to improve patient outcomes.