Prevention of Cardioembolic Stroke - Dr Jeremy Chow
1.
Prevention of CardioembolicStroke in 2025
PRESENTED BY:
DR JEREMY CHOW
Consultant Cardiologist & Electrophysiologist
Director of Electrophysiology Service
MBBS, M.Med (Int Med), FAMS
FRCP (London), FESC, FHRS, FAsCC
Certified Cardiac Device Specialist
Website: www.ahvc.com.sg
Email: drchow.jeremy@ahvc.com.sg
2.
AHVC ASM 16August 2025
Where do the clots come from?
3.
AHVC ASM 16August 2025
So How Can We Prevent Cardioembolic Stroke?
1. Restore AF to Sinus Rhythm
Antiarrhythmic vs Ablation to maintain SR
2. Prevent blood clot formation in LAA
Anticoagulation vs LAAC
3. PFO Closure in young stroke patients?
4.
Case – MrVA
35 year old Executive Chef
No CV Risk Factor
Saw me in 2020 for second opinion.
Presented with left sided transient
numbness with transient loss of tone.
No facial asymmetry
MRI confirmed right parietal, occipital
and frontal subacute infarcts. MRA
normal.
5.
Case – MrVA
Did 72H telemetry monitoring- No AF
24H Holter - No AF
First TTE with bubble - negative
US carotid – No plaque or stenosis.
Transcranial doppler bubble study
showed - positive for right to left
shunt
Auto-immune screen negative
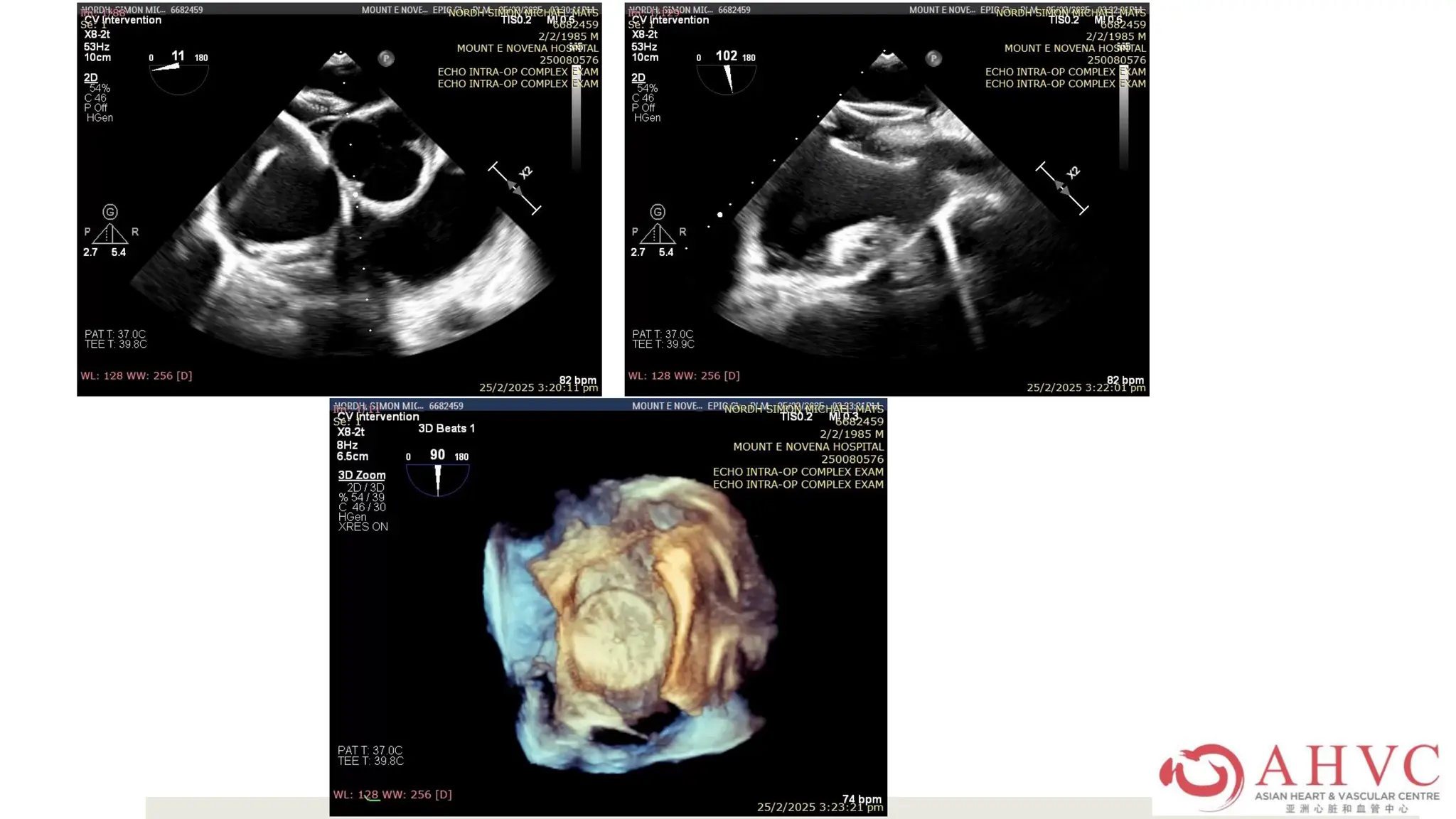
7.
What are highrisk PFO?
➢ Current evidence indicates that patients with moderate/large PFOs or
atrial septal aneurysm (ASA) have a higher risk of stroke recurrence
and are more likely to benefit from PFO closure.
➢ The size of the PFO is often quantified by the number of bubbles that
cross into the left atrium. A large PFO has been defined as the
appearance of more than 20 microbubbles in the left atrium within 3
cardiac cycles after opacification of the right atrium.
➢ An ASA is defined as a septum primum excursion ≥10 mm from the
plane of the atrial septum into the right atrium or left atrium and is also
considered a high-risk feature.
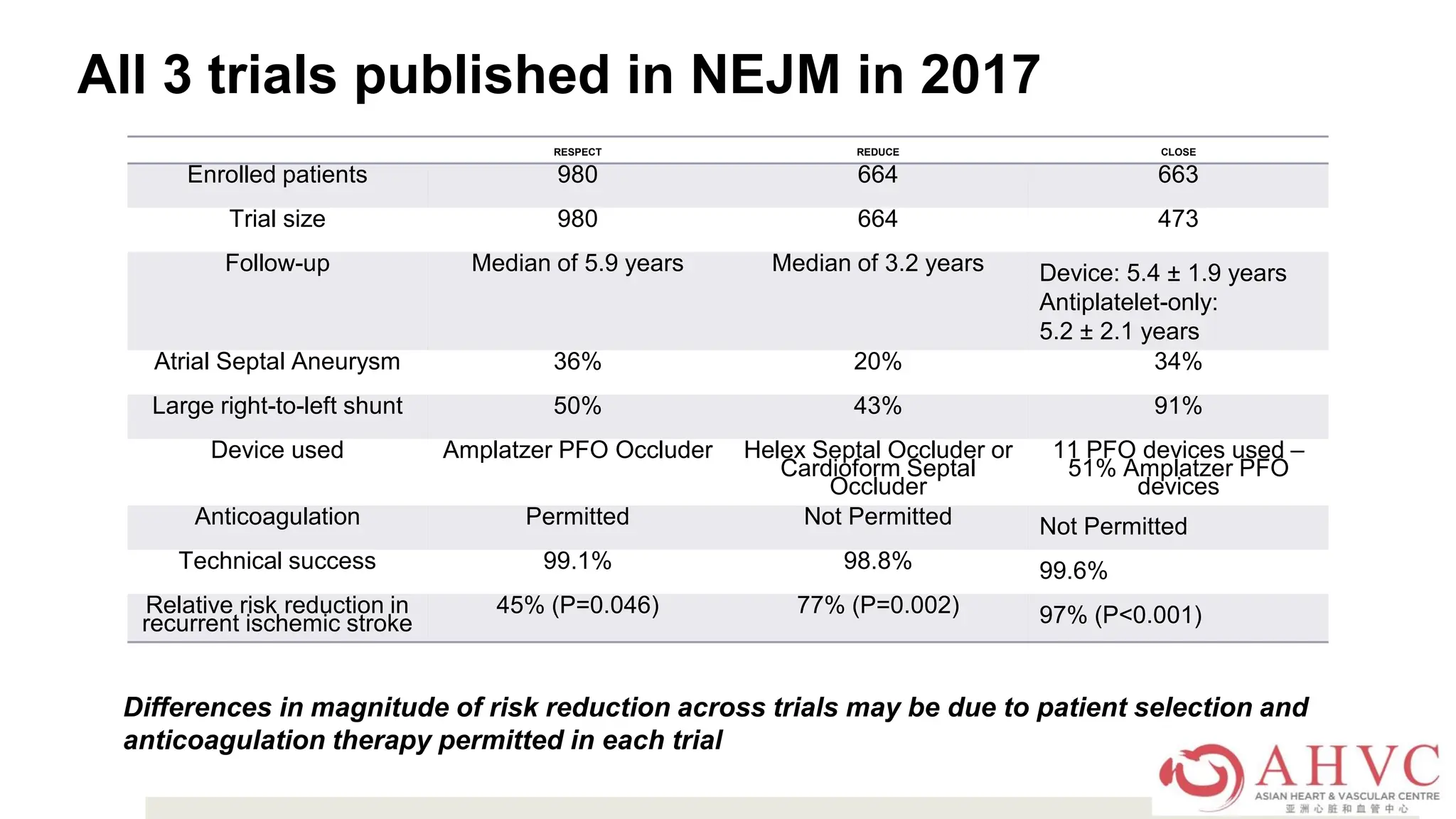
RESPECT REDUCE CLOSE
Enrolledpatients 980 664 663
Trial size 980 664 473
Follow-up Median of 5.9 years Median of 3.2 years Device: 5.4 ± 1.9 years
Antiplatelet-only:
5.2 ± 2.1 years
Atrial Septal Aneurysm 36% 20% 34%
Large right-to-left shunt 50% 43% 91%
Device used Amplatzer PFO Occluder Helex Septal Occluder or
Cardioform Septal
Occluder
11 PFO devices used –
51% Amplatzer PFO
devices
Anticoagulation Permitted Not Permitted Not Permitted
Technical success 99.1% 98.8% 99.6%
Relative risk reduction in
recurrent ischemic stroke
45% (P=0.046) 77% (P=0.002) 97% (P<0.001)
Differences in magnitude of risk reduction across trials may be due to patient selection and
anticoagulation therapy permitted in each trial
All 3 trials published in NEJM in 2017
How about olderpatients? > 60 yo
(1) the procedural success rate was high (99.9%) and major procedural-related
complications low (<2%), similar to their younger counterparts;
(2) the incidence of cerebrovascular ischemic events after a median follow-up
of 3 years was lower than expected according to the RoPE score in the older
group (<1 and <2 per 100 patient-years for stroke and stroke/TIA,
respectively) but higher compared to that observed in younger PFO closure
patients; and
(3) the rate of new-onset AF after the procedure was 2.66 per 100 patient-
years, higher than expected compared to the general population of the
same age.
AHVC ASM 16August 2025
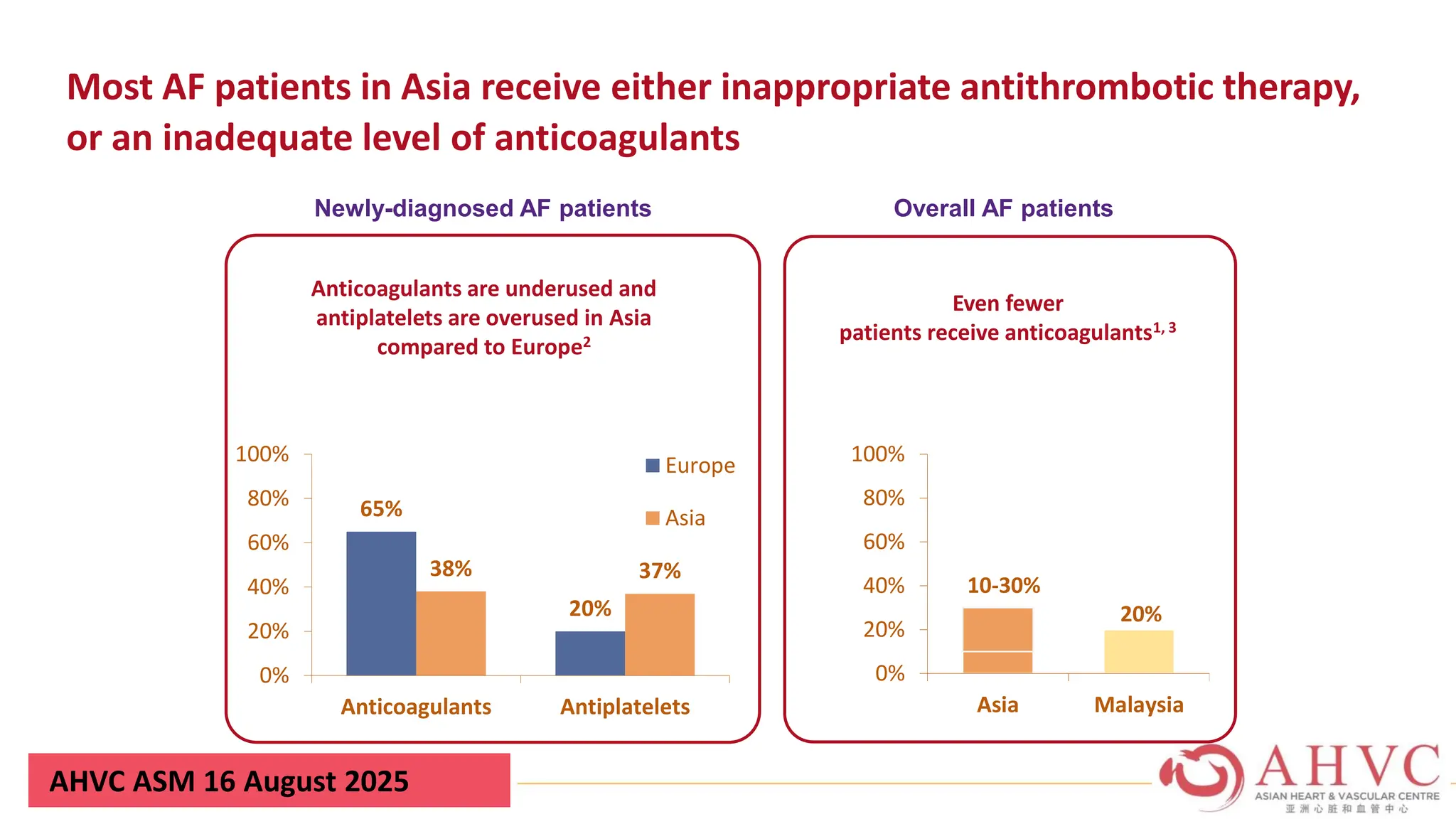
Most AF patients in Asia receive either inappropriate antithrombotic therapy,
or an inadequate level of anticoagulants
Proportion on anticoagulants or antiplatelets
by region
Proportion on anticoagulants
Newly-diagnosed AF patients Overall AF patients
Anticoagulants are underused and
antiplatelets are overused in Asia
compared to Europe2
65%
20%
38% 37%
0%
20%
40%
60%
80%
100%
Anticoagulants Antiplatelets
Europe
Asia
10-30%
20%
0%
20%
40%
60%
80%
100%
Asia Malaysia
Even fewer
patients receive anticoagulants1, 3
21.
AHVC ASM 16August 2025
Even in Singapore according to the GARFIELD Registry
Antithrombotic treatment according to CHA2DS2-VASc score, Singapore (N=70)
22.
AHVC ASM 16August 2025
• Took more than 10 years to plan
• Nearly 5k patients recruited from 105
centres in 27 countries
• Final follow-up in March 2021
• Mean follow-up – 3.8 years
Validating the concept of closing the left
atrial appendage to prevent stroke
23.
Case – MrCKK
60 year old Lawyer
CV Risk Factor – Hypertension,
Hyperlipidaemia
Hx of Chronic AF since 2018 on
rate control and anticoagulation
Hx of OSA on CPAP
Saw me in 2021 for second opinion
24.
Case – MrCKK
He was planned for EPS ablation
in July 2021.
CTCA done in June showed
minor CAD and no LAA clot.
His Xarelto was stopped for 1
day and he had TEE prior to EPS.
New LAA clot.
25.
Case – MrCKK
He was planned for EPS ablation
in July 2021.
CTCA done in June showed
minor CAD and no LAA clot.
His Xarelto was stopped for 1
day and he had TEE prior to EPS.
New LAA clot.
27.
Case – MrCKK
After LMWH for 6 weeks, he came
back for EPS AF in Dec 2021 and
had successful PVI.
He was in paroxysmal AF post
ablation but his NYHA improved.
In April 2022, he had recurrence of
persistent AF. He was admitted for
cardioversion.
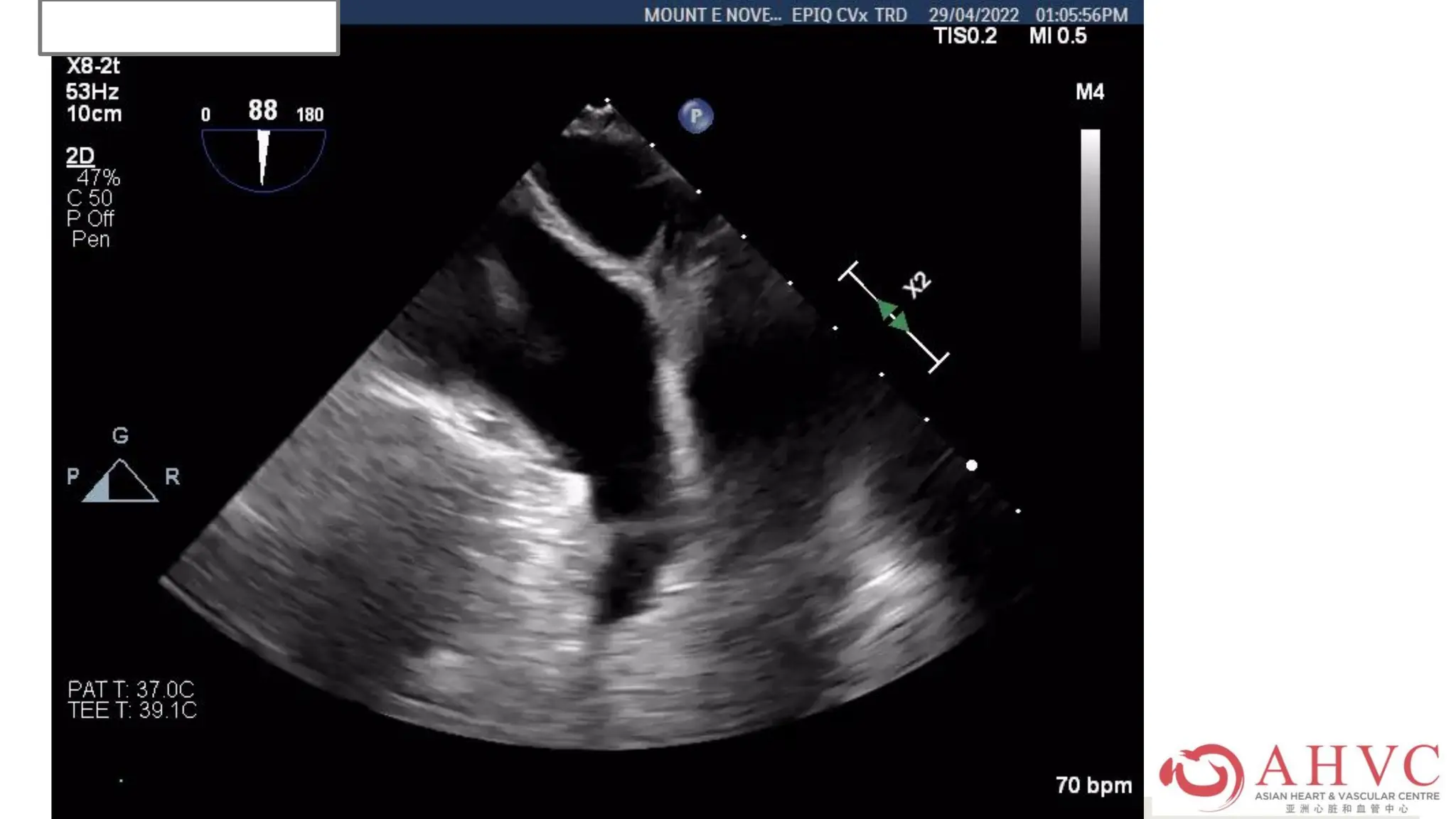
28.
Case – MrCKK
TEE was done before
cardioversion which showed no
clot in LAA.
His Lixiana was uninterrupted.
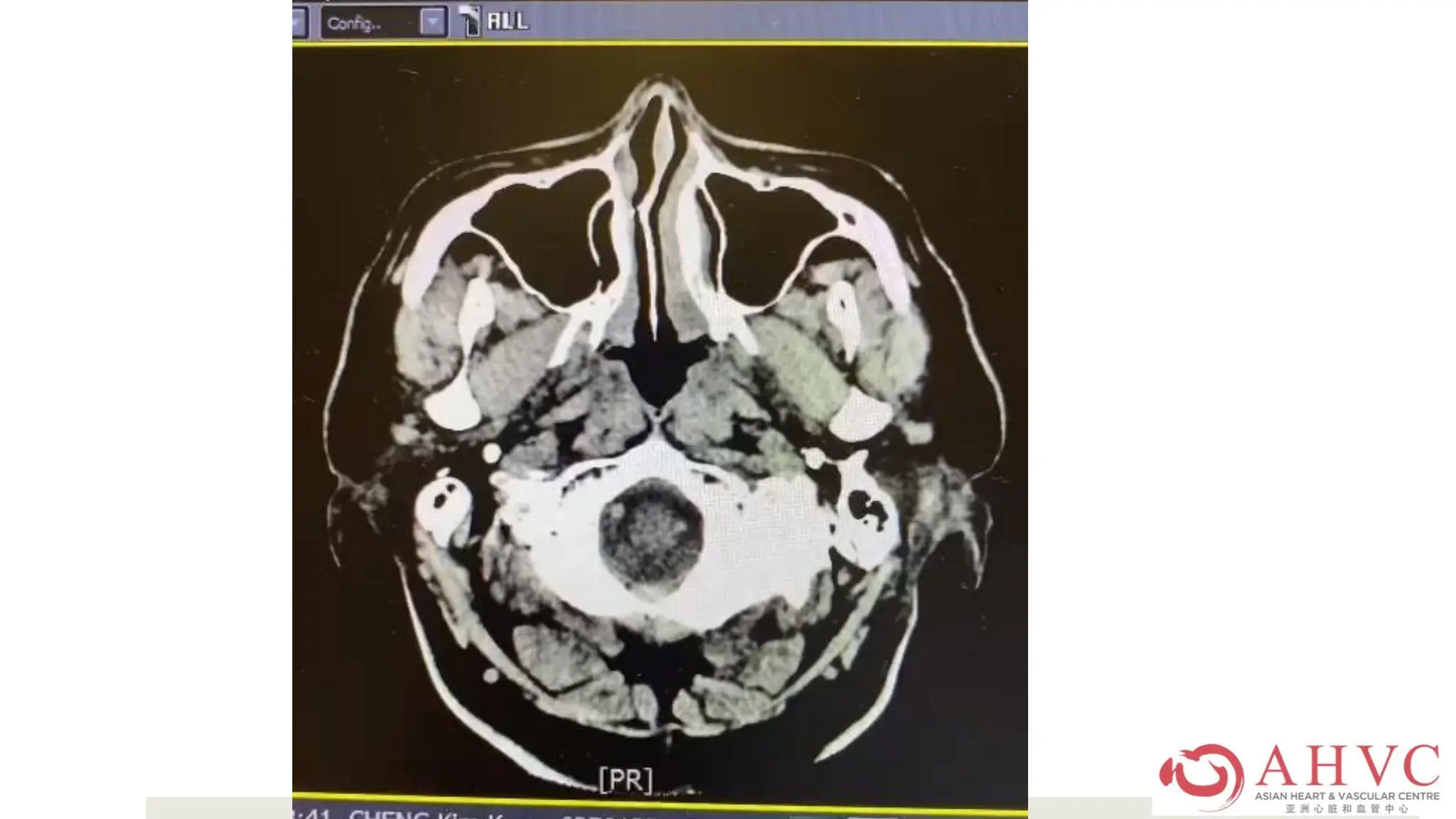
30.
Case – MrCKK
Cardioversion was successful, he
was planned for home the next
morning when he suddenly had
acute vertigo with incoordination.
MRI showed acute right cerebellar
stroke.
Now what can I do? Stroke despite
DOAC
35.
AHVC ASM 16August 2025
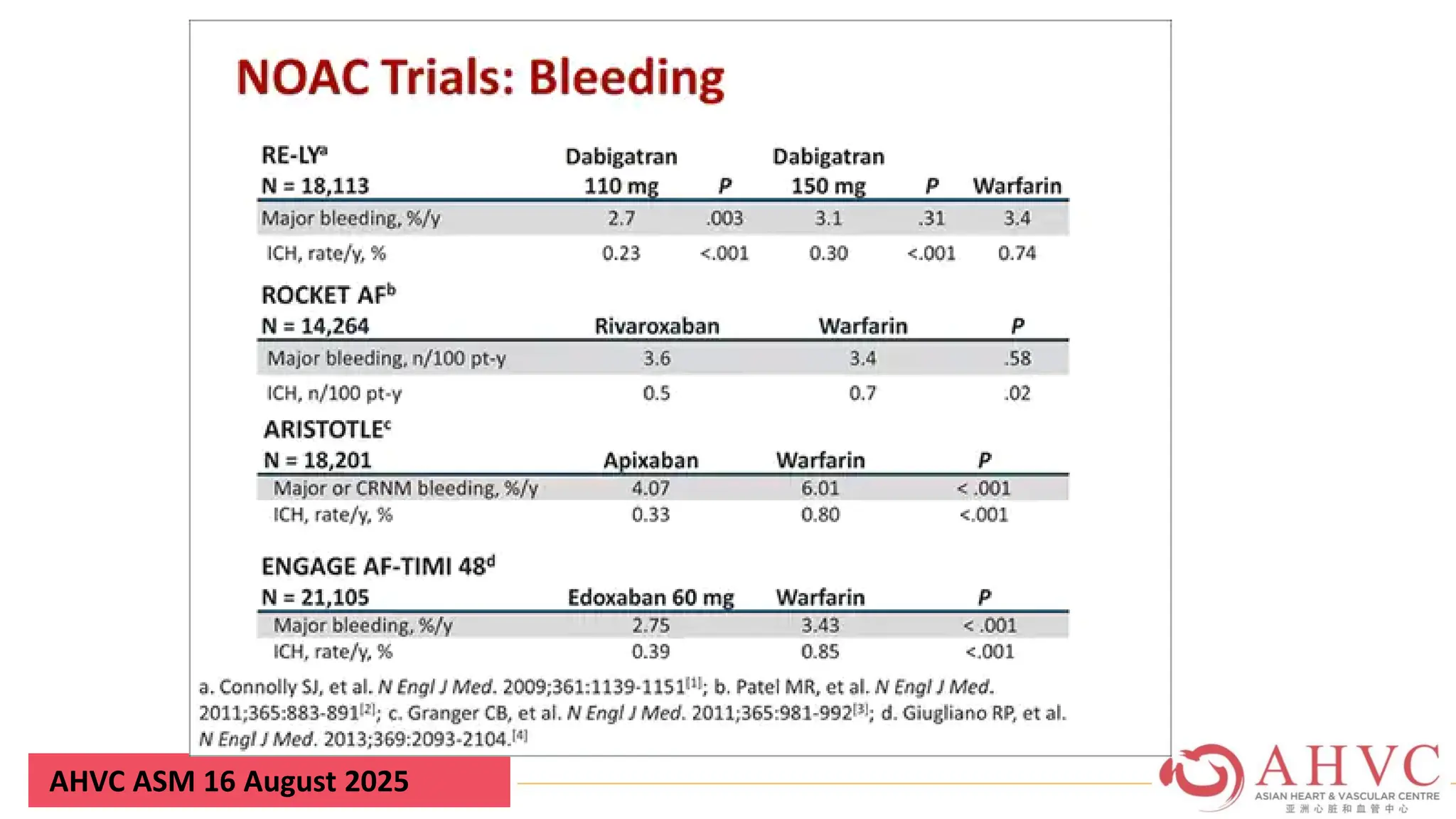
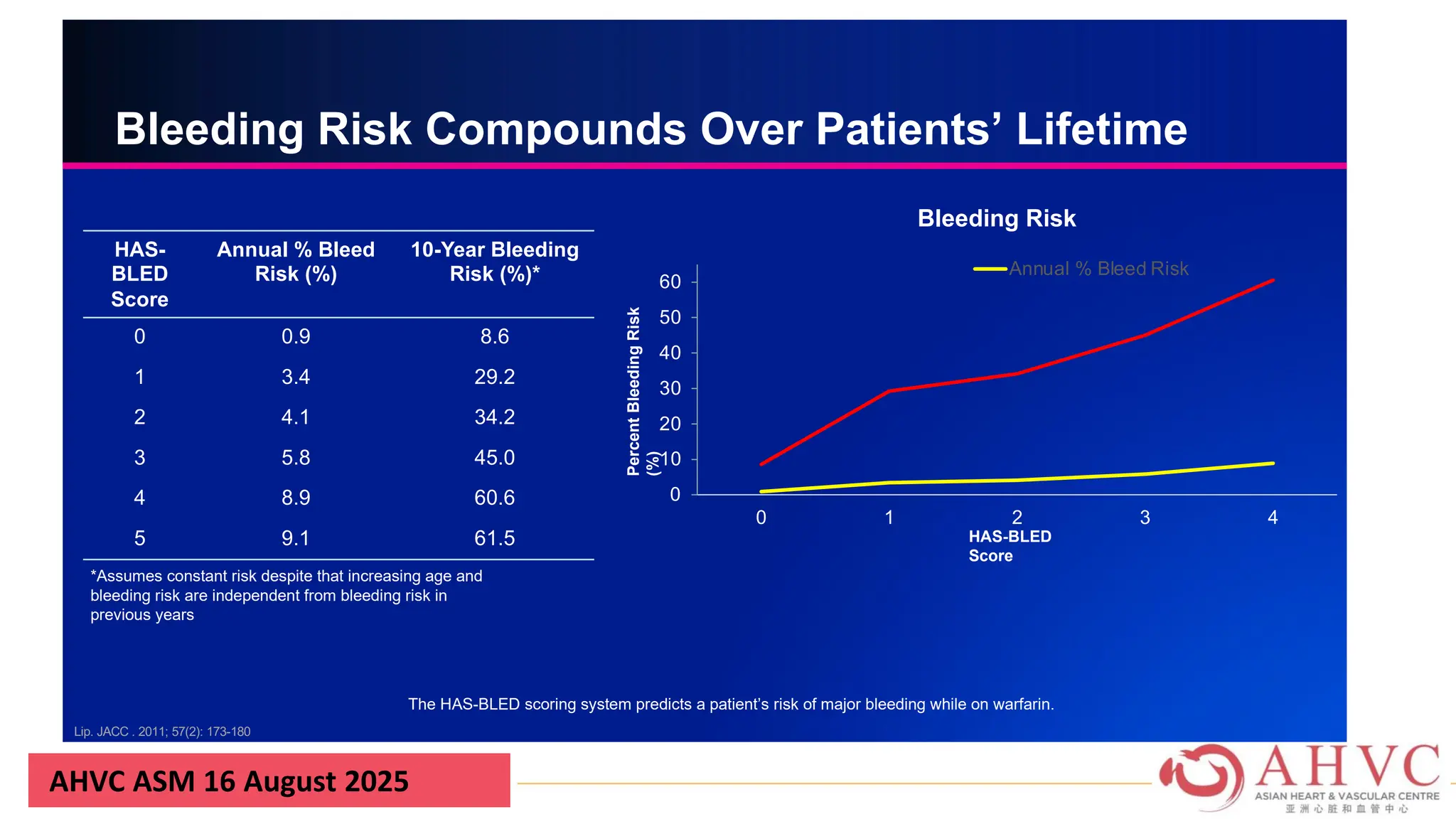
Is LAAC Superior to anticoagulation?
1. Cumulative bleeding risk of DOAC
2. Cost effectiveness of LAAC
3. Mortality benefit ?
AHVC ASM 16August 2025
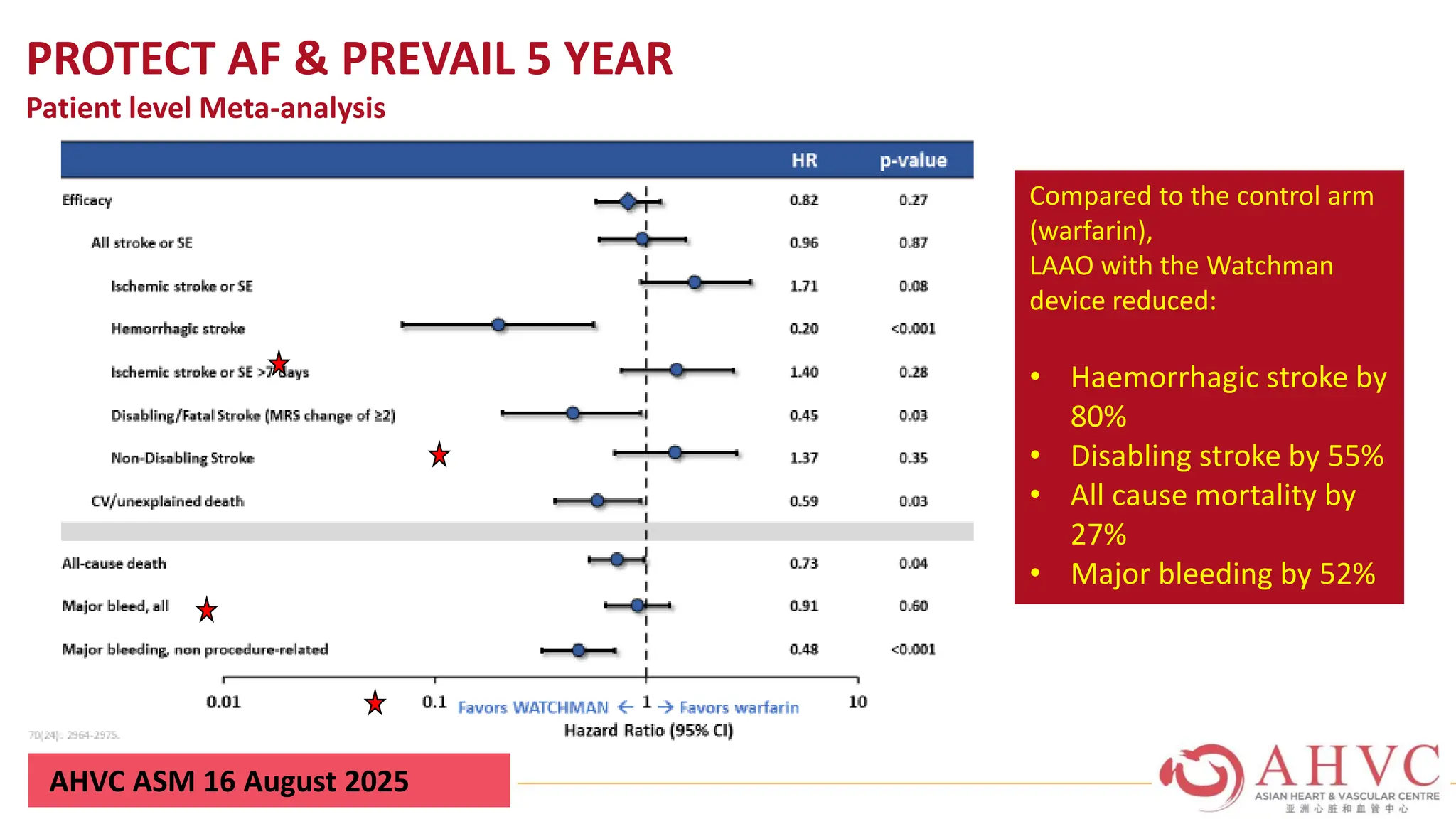
PROTECT AF & PREVAIL 5 YEAR
Patient level Meta-analysis
Compared to the control arm
(warfarin),
LAAO with the Watchman
device reduced:
• Haemorrhagic stroke by
80%
• Disabling stroke by 55%
• All cause mortality by
27%
• Major bleeding by 52%
Take Home Message….
Highrisk PFO should be closed in young
patients < 60 yo.
LAAC is superior to DOAC if we want to
achieve - less bleeding with similar degree
of stroke prevention in the long term.
LAAC is the more cost-effective treatment in
stroke prevention.