Downloaded 314 times
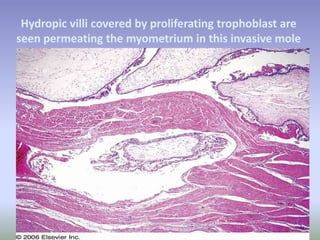
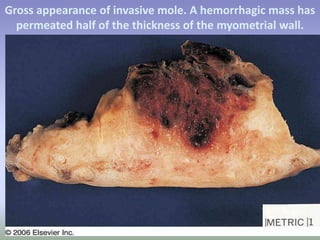
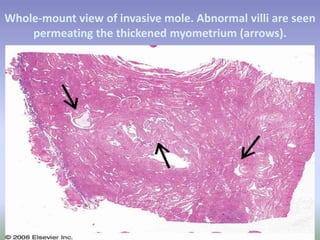

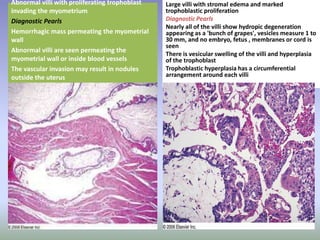
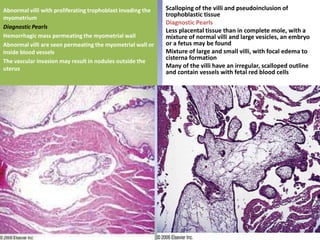
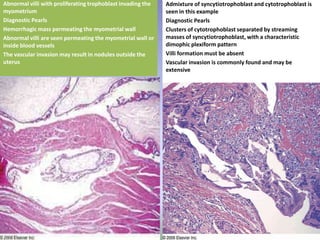
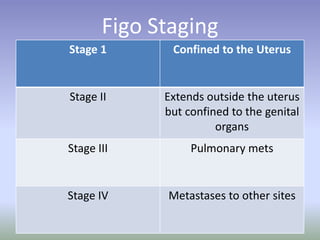

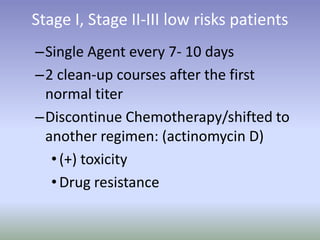
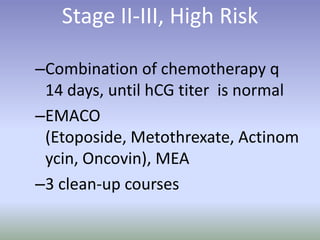


Invasive mole is a complication of molar pregnancy where abnormal villi grow into the myometrium or blood vessels. It occurs in approximately 15% of complete moles and can metastasize to other organs. Clinical features include persistent hemorrhage and uterine perforation. Microscopically, proliferating trophoblast tissue is seen invading the myometrium. Treatment involves chemotherapy, with single or combination drug regimens depending on the disease stage. The goals are to normalize hCG levels and administer additional "clean-up" courses of chemotherapy.










































































