Downloaded 94 times











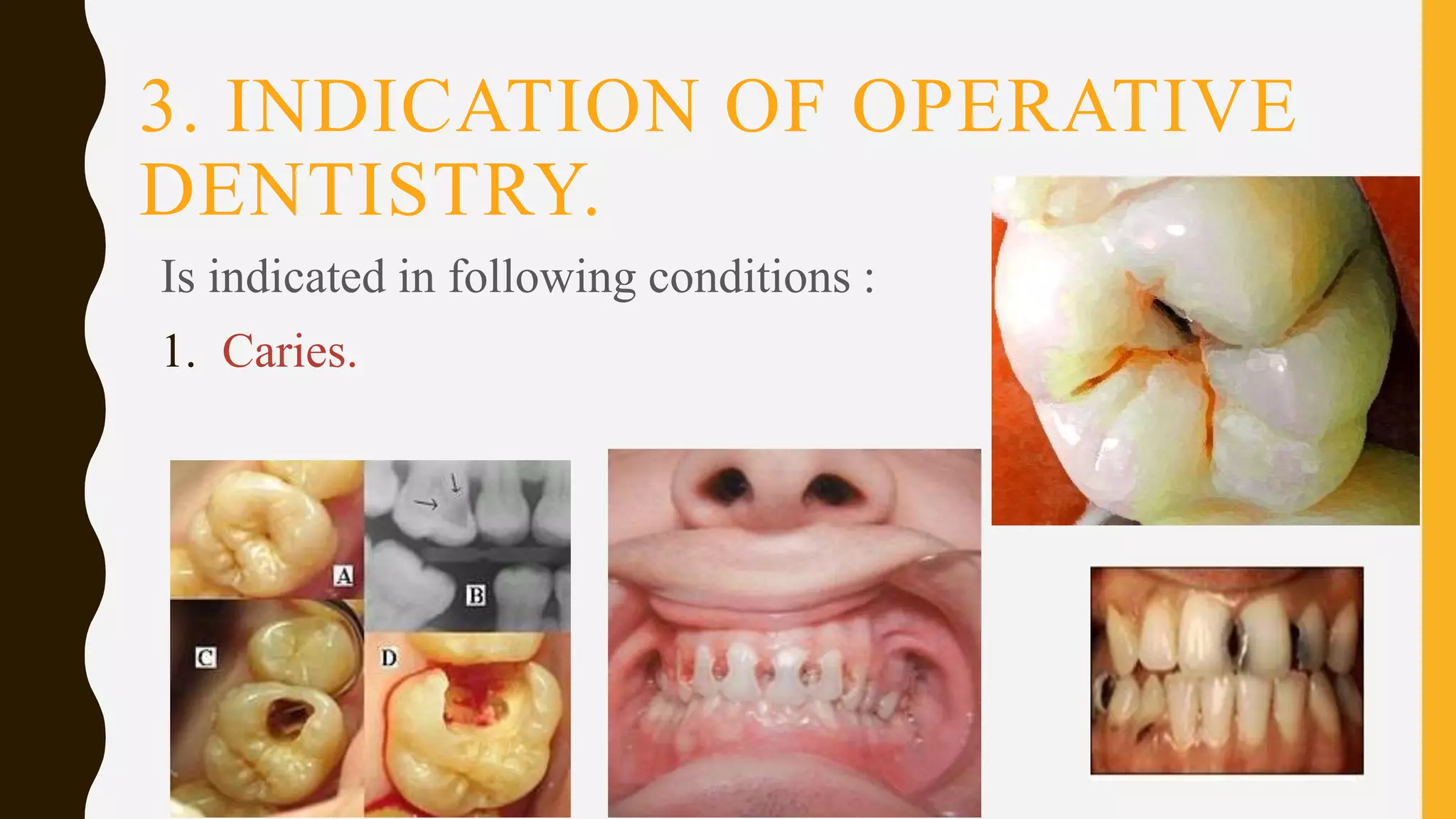

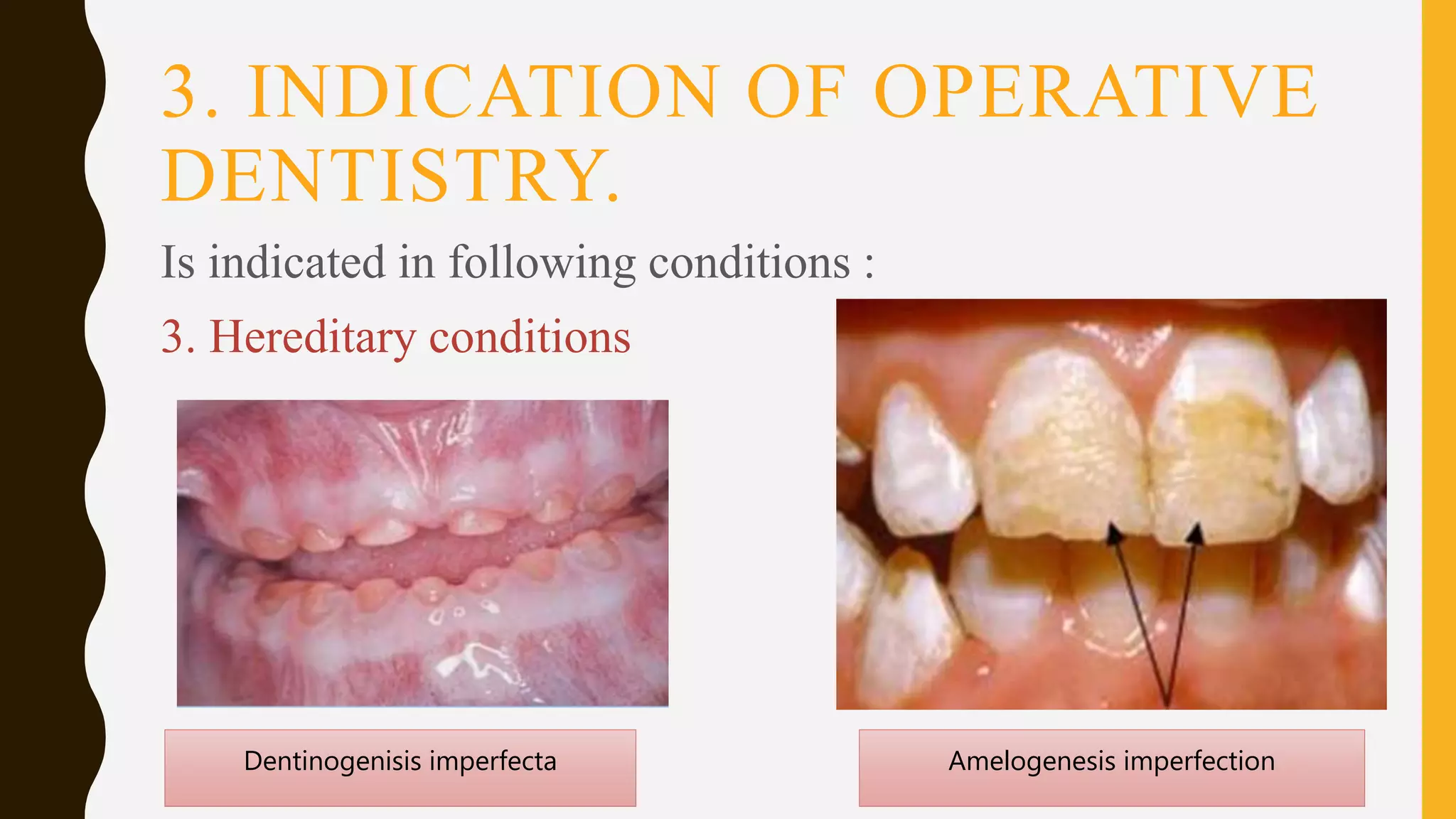

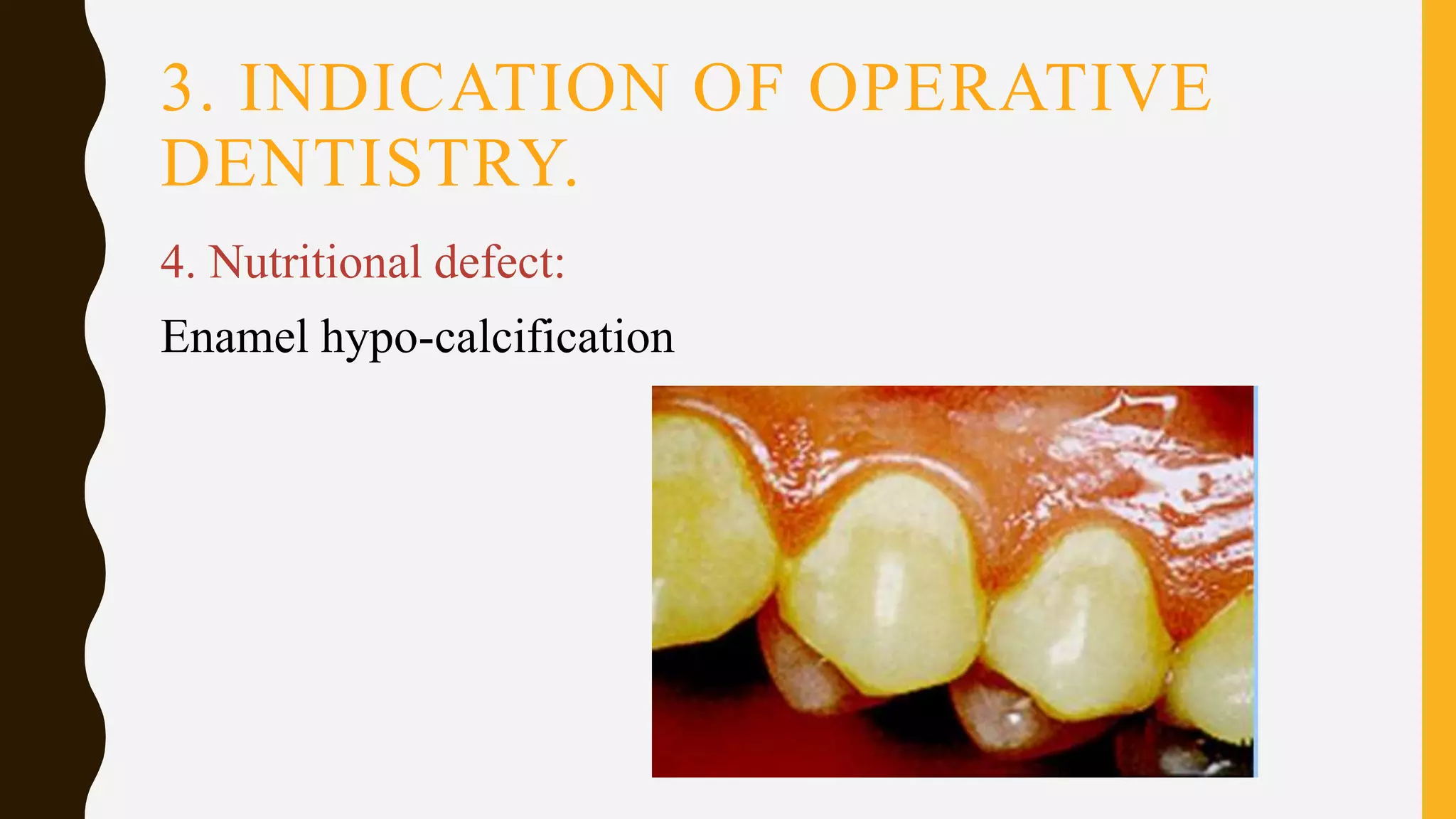

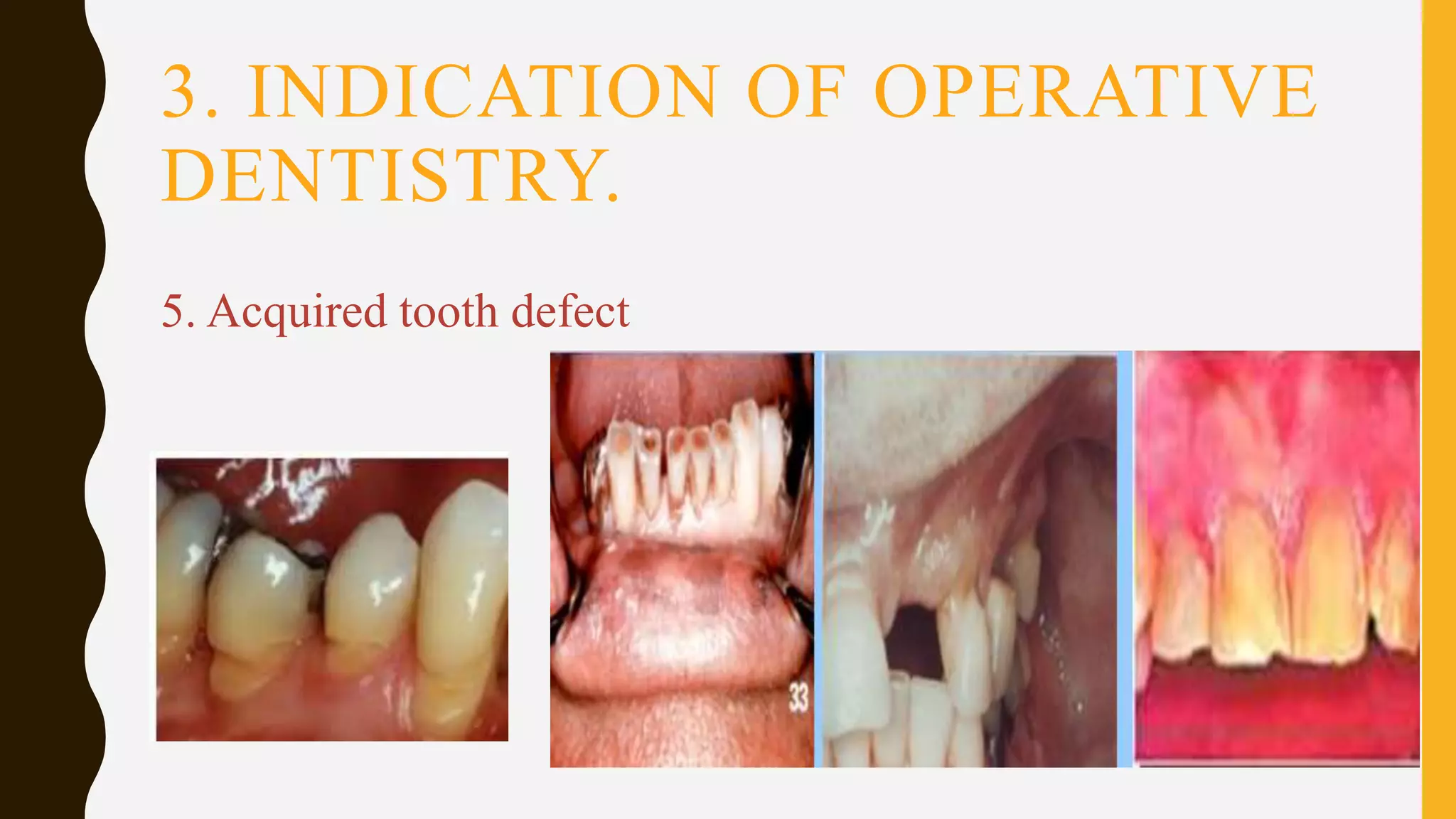

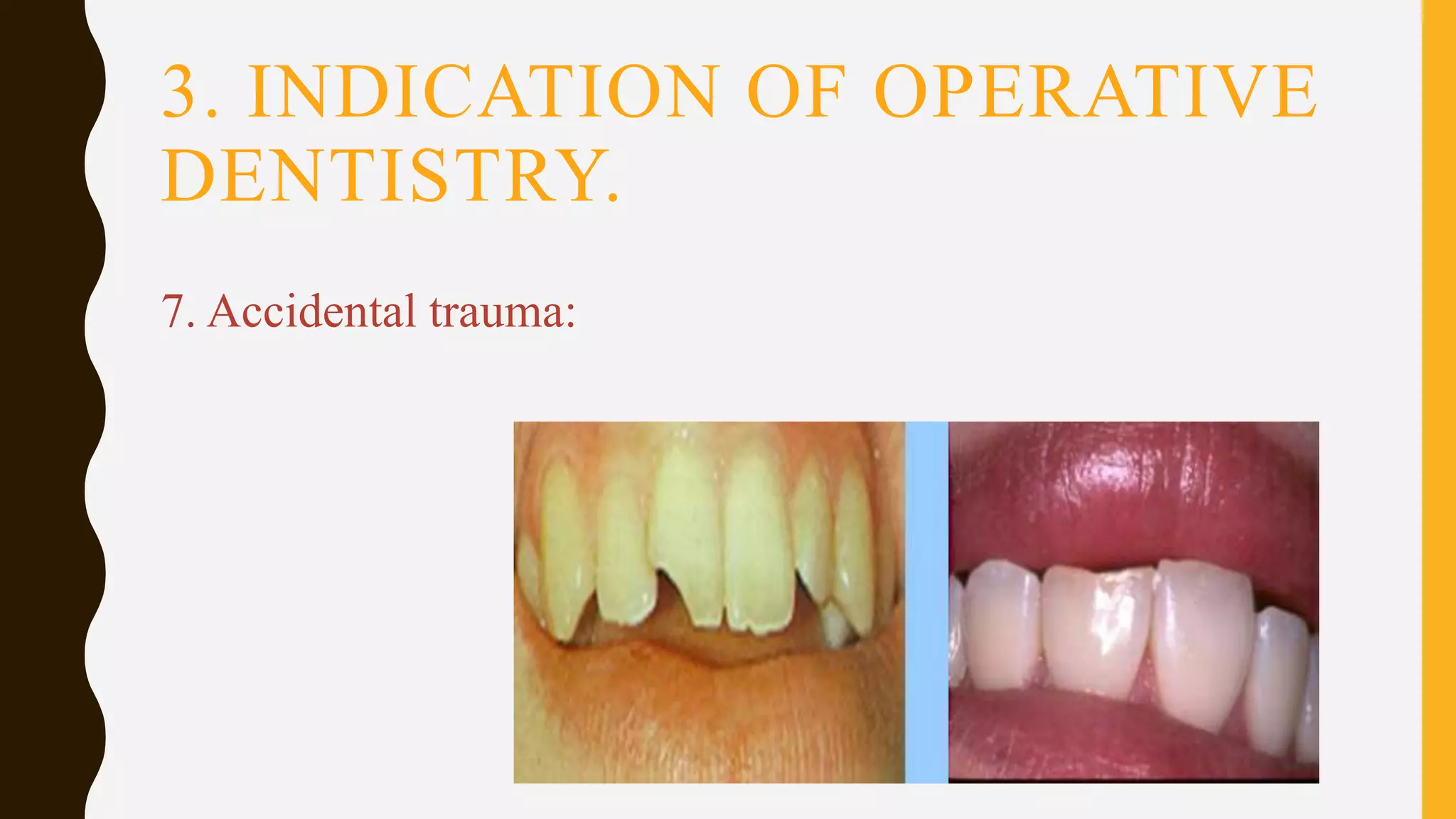
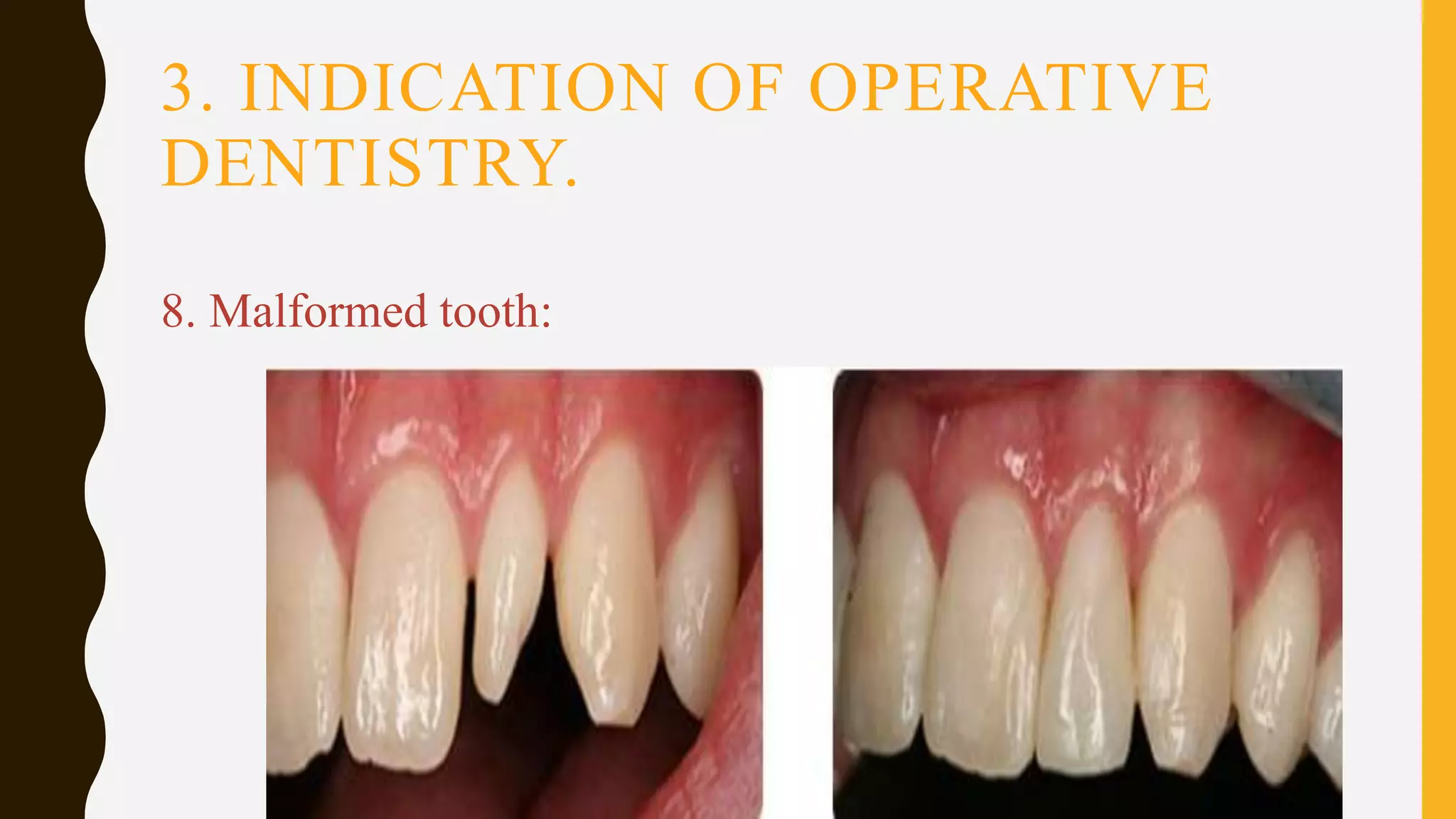
















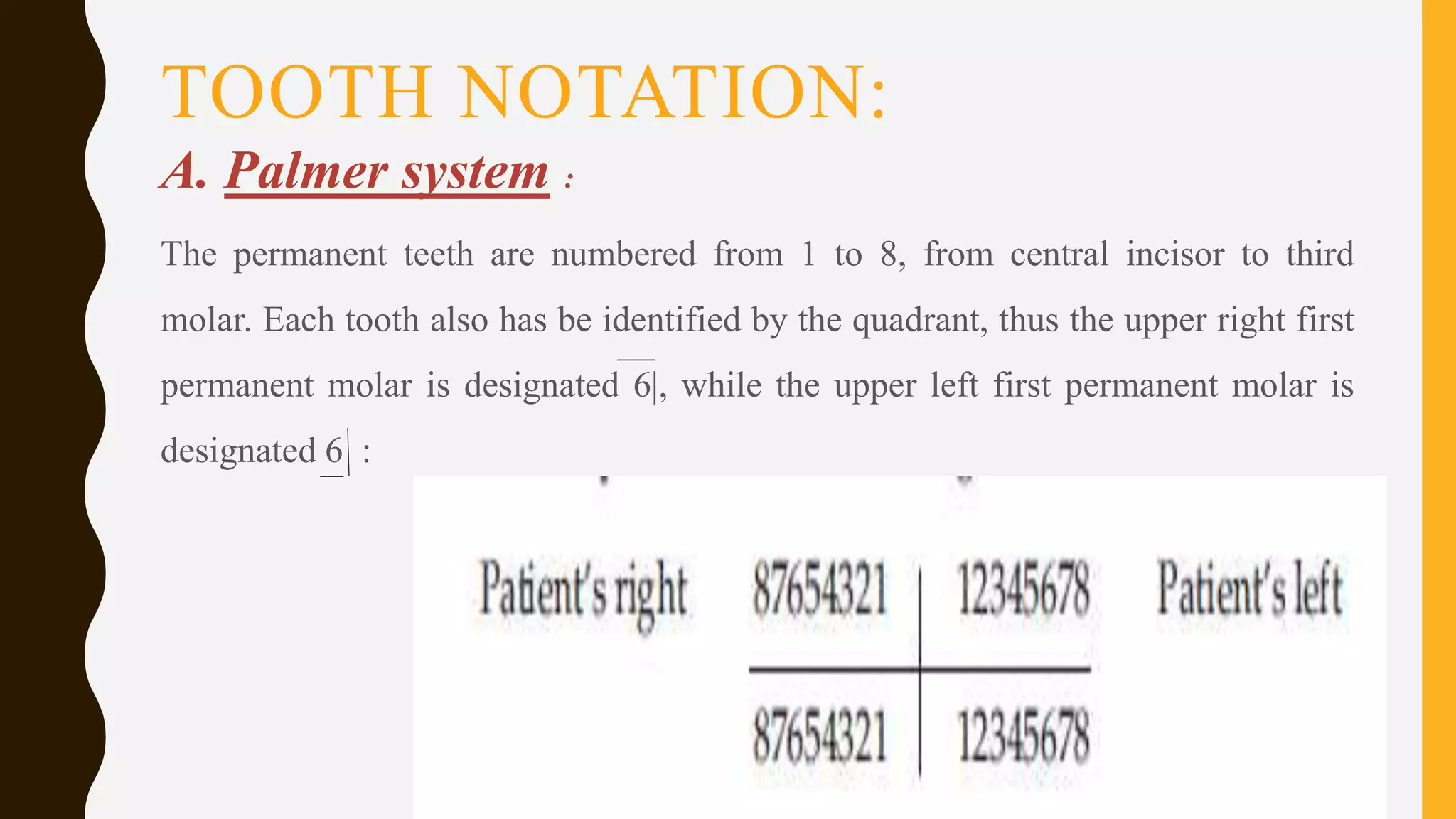
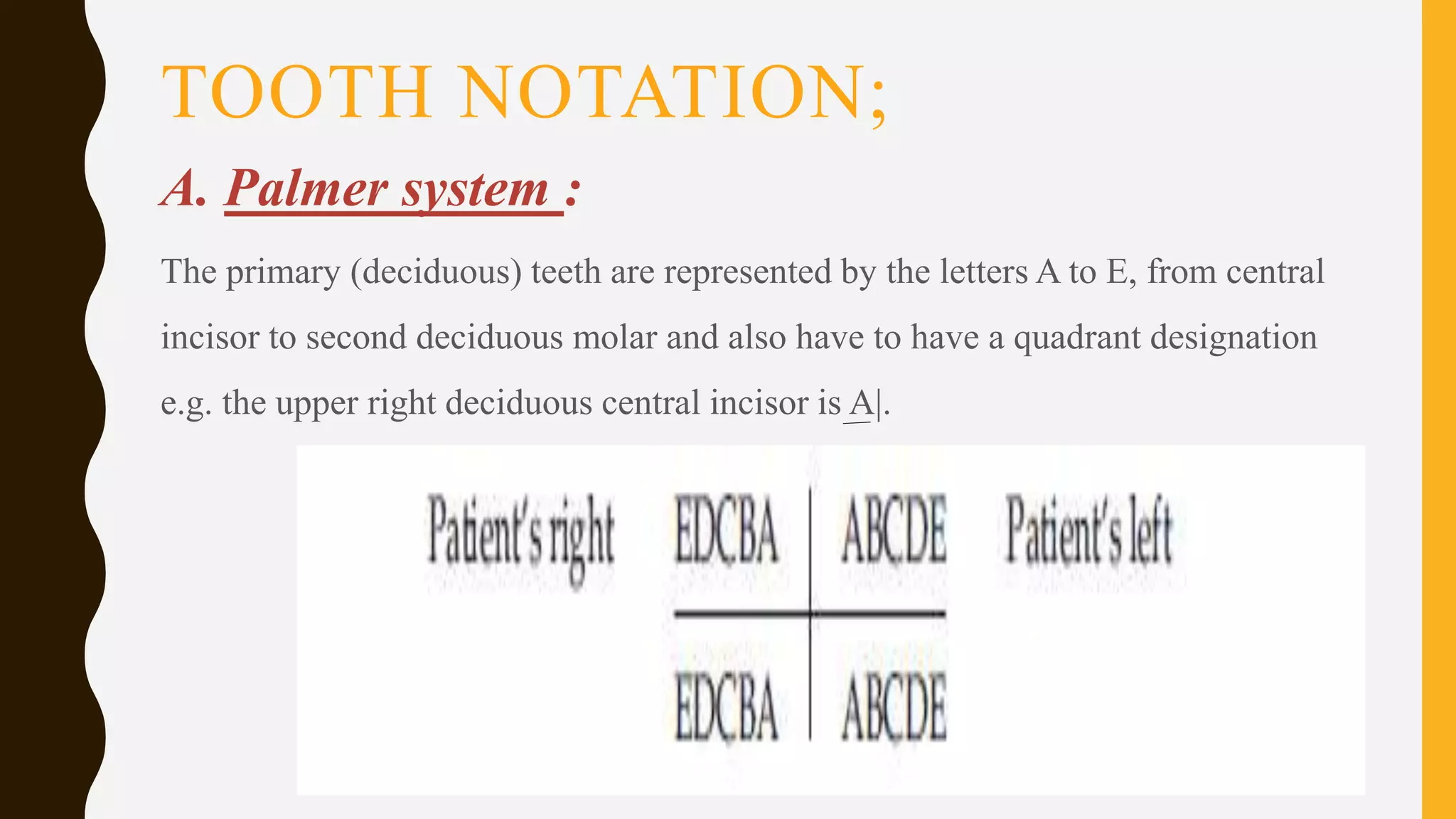
















Operative dentistry deals with the diagnosis, prevention, and restoration of tooth structure to correct defects, restore function and aesthetics. The history of operative dentistry began with tooth extractions in the middle ages and has evolved to be more evidence-based and focused on minimally invasive techniques. It is indicated to treat conditions like dental caries, trauma, and developmental defects. Its main objectives are diagnosis, prevention, preservation and restoration of teeth. There are different systems for notation of individual teeth, with the most commonly used systems being the Universal system and FDI (Federation Dentaire Internationale) two-digit system.