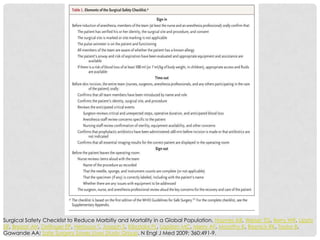
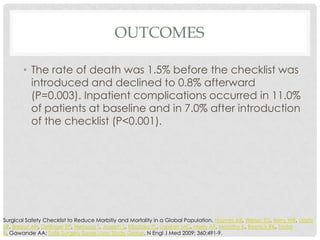
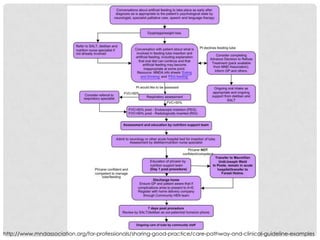
This document discusses interprofessional rounding teams and strategies to improve teamwork and communication. It provides background on how interprofessional healthcare teams can improve patient outcomes. Checklists, care pathways, and interprofessional education are presented as potential solutions. Checklists have been shown to reduce medical errors and mortality. Care pathways, while challenging to implement, can standardize care and reduce prescribing errors. Brief interprofessional education sessions have been found to improve collaboration attitudes and skills among professionals. Overall, the document advocates for interprofessional rounding teams and strategies to enhance communication and teamwork across disciplines.