Download to read offline





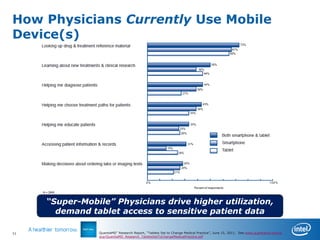
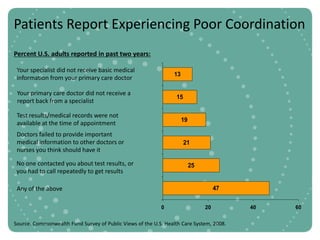
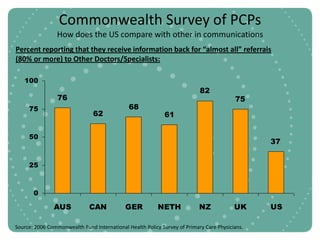
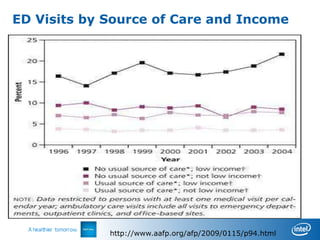
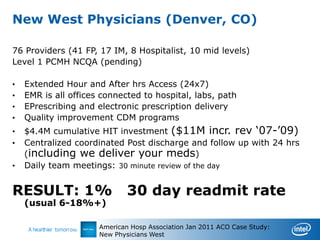
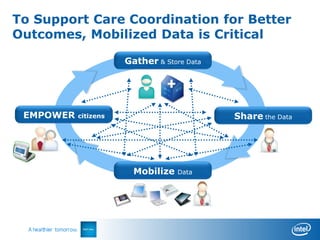

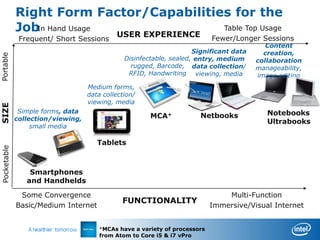


This document discusses the importance of collaborative care and care coordination for healthcare delivery systems. It notes that solo practice is no longer a sustainable business model and that fee-for-service payments have limitations. The document provides evidence that care coordination can reduce costs through fewer hospital admissions and readmissions without worse health outcomes. It also shows that patients experience a lack of communication and information sharing between their different doctors. To improve care coordination, mobile access to patient data and collaborative workflows are seen as critical, as mobile devices are increasingly how physicians access information. The right devices and secure mobile computing are needed to enable these new care coordination models.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









