Download to read offline



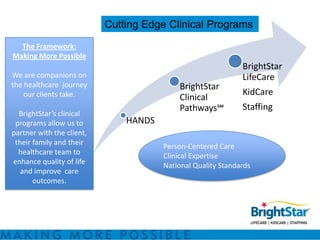
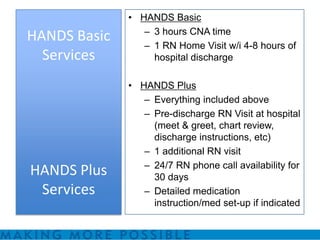

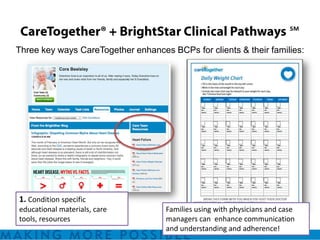
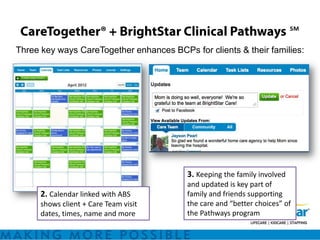
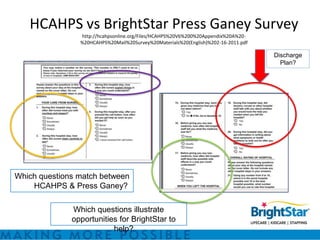

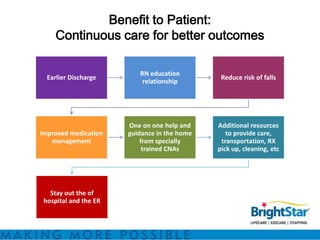
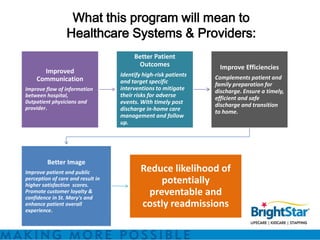



BrightStar offers private duty home care programs like HANDS and Clinical Pathways to reduce hospital readmissions and improve quality of life. HANDS provides home care after discharge to address issues that arise. Clinical Pathways is a condition-specific, transitional care program focused on reducing negative outcomes and optimizing quality of life through RN visits, education, and monitoring. These programs aim to address the top reasons for readmissions like medication management and lack of home support. They utilize technology, evidence-based practices, and specially trained staff to benefit patients, healthcare systems, and providers through better outcomes and efficiencies.







![resume 2013[1][1]](https://cdn.slidesharecdn.com/ss_thumbnails/8ad77ac3-587d-4643-8b4a-6947b2902cfc-150209201327-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)





































