Downloaded 52 times


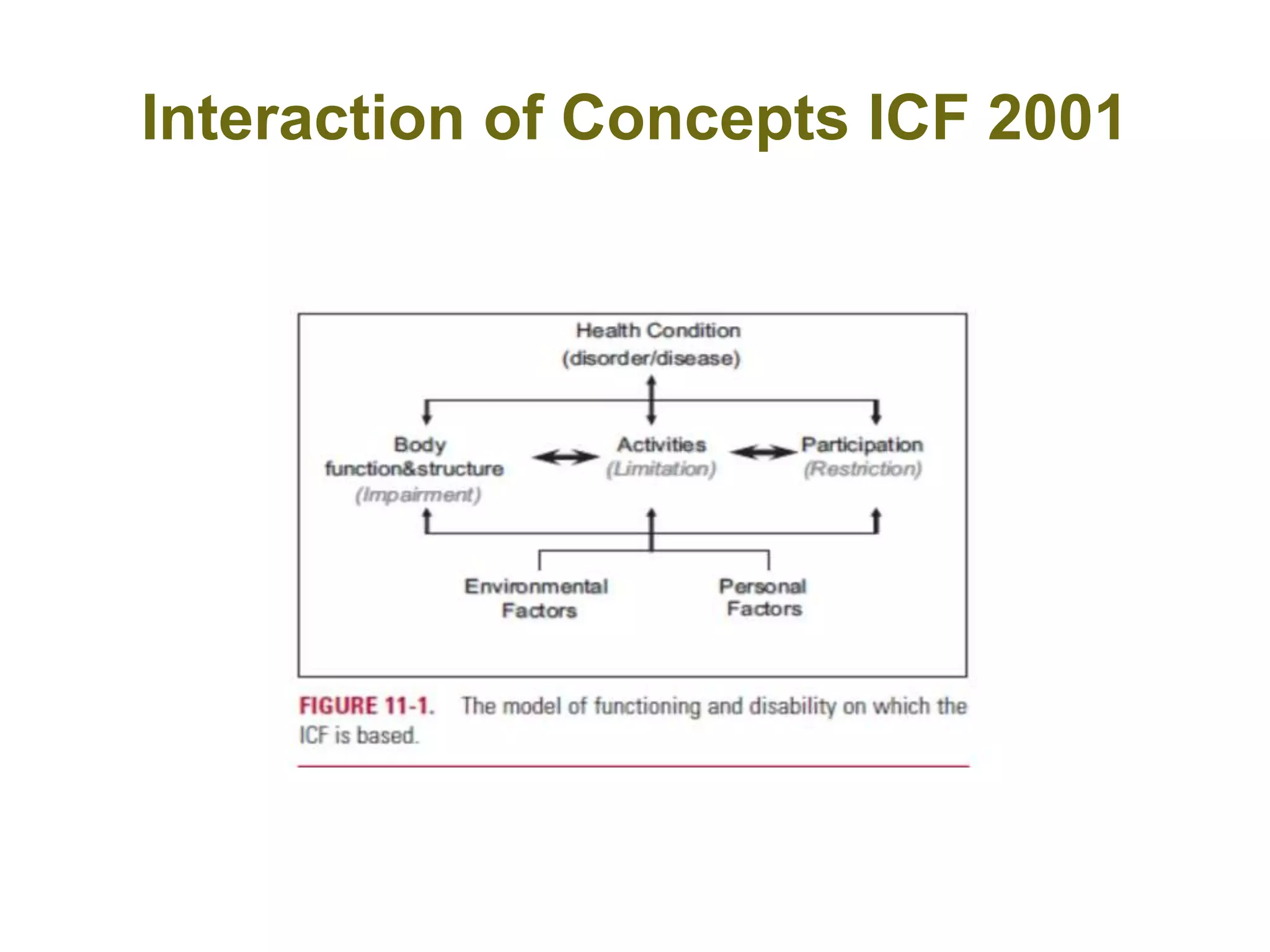
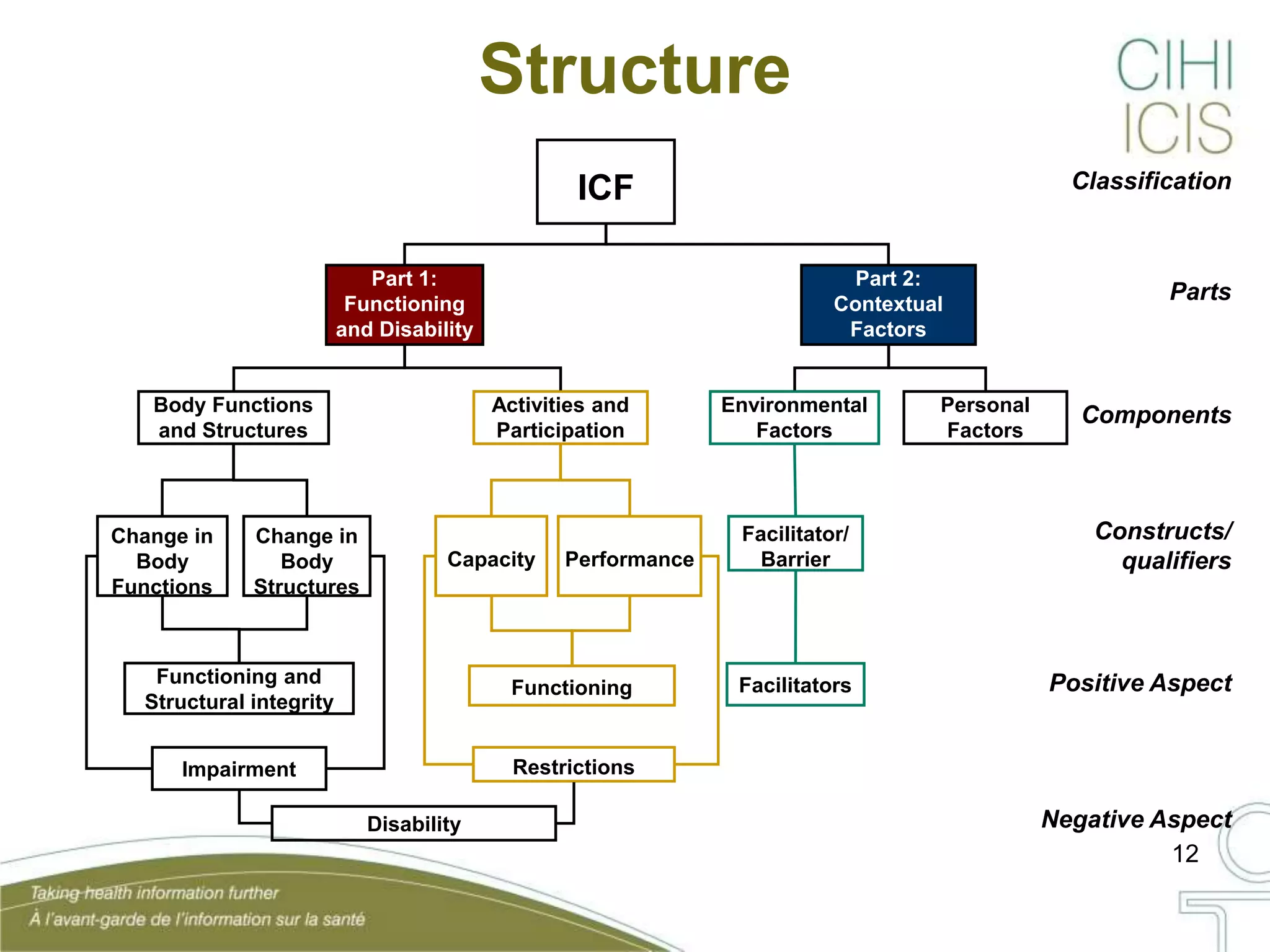
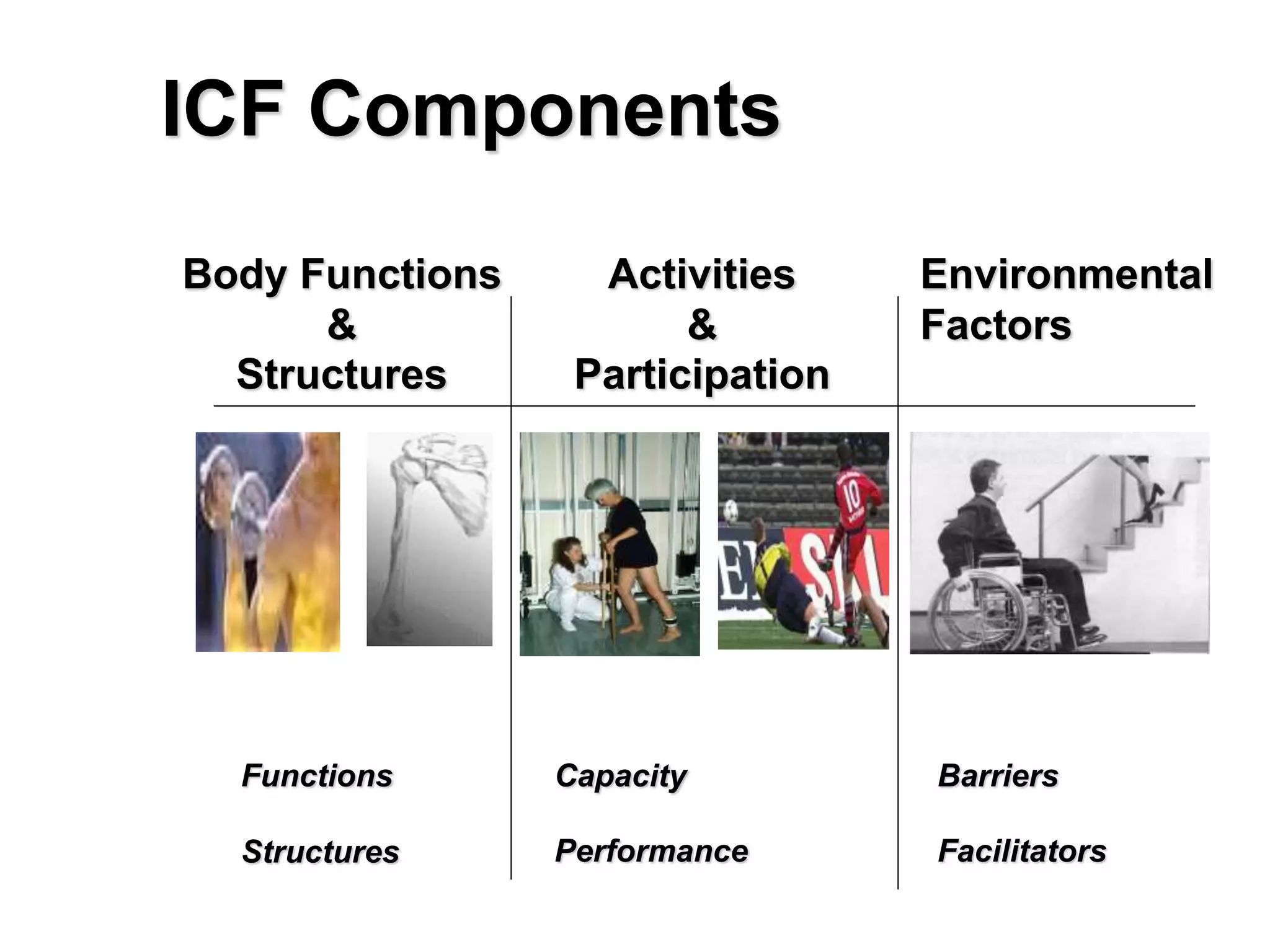
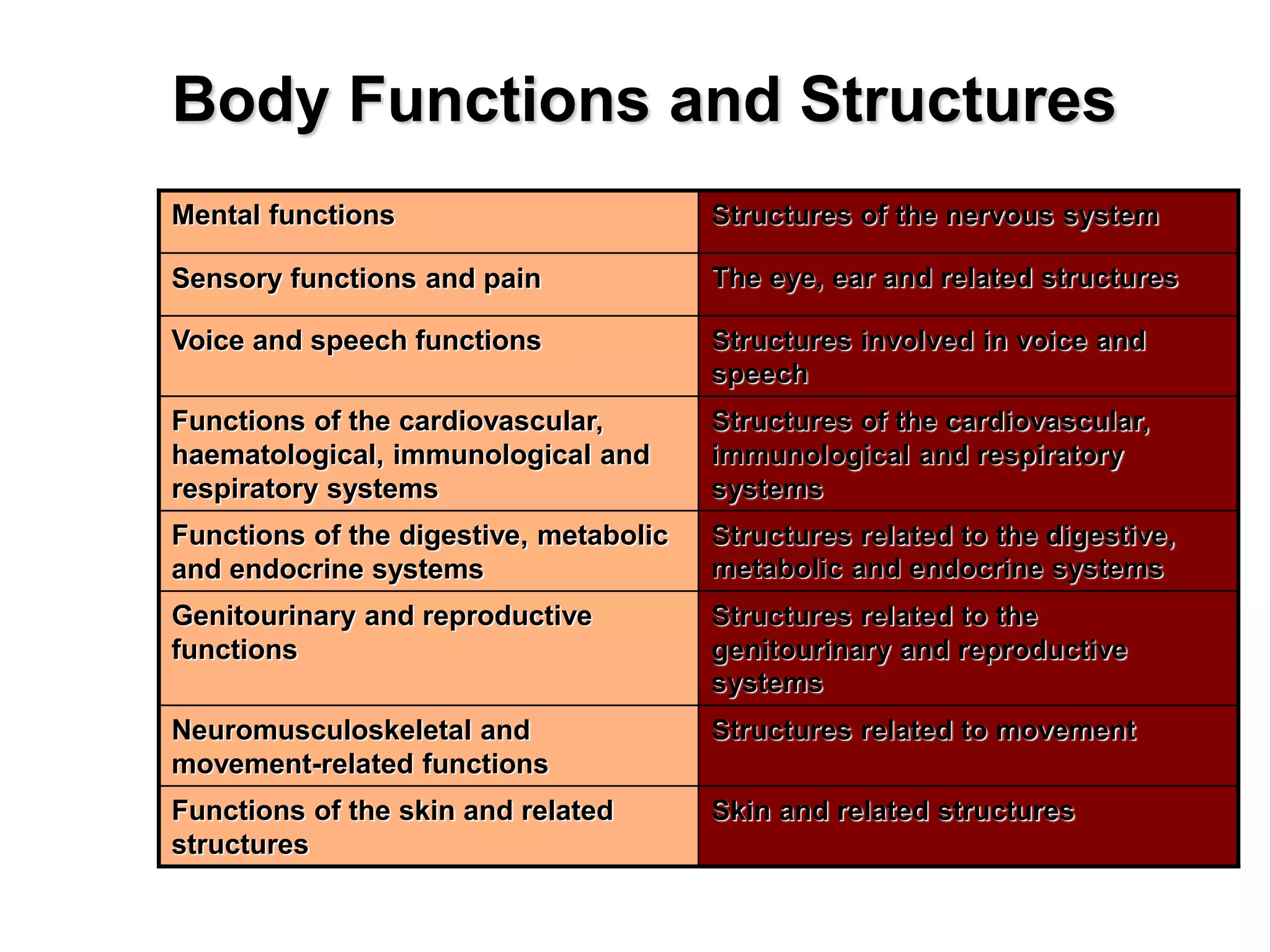
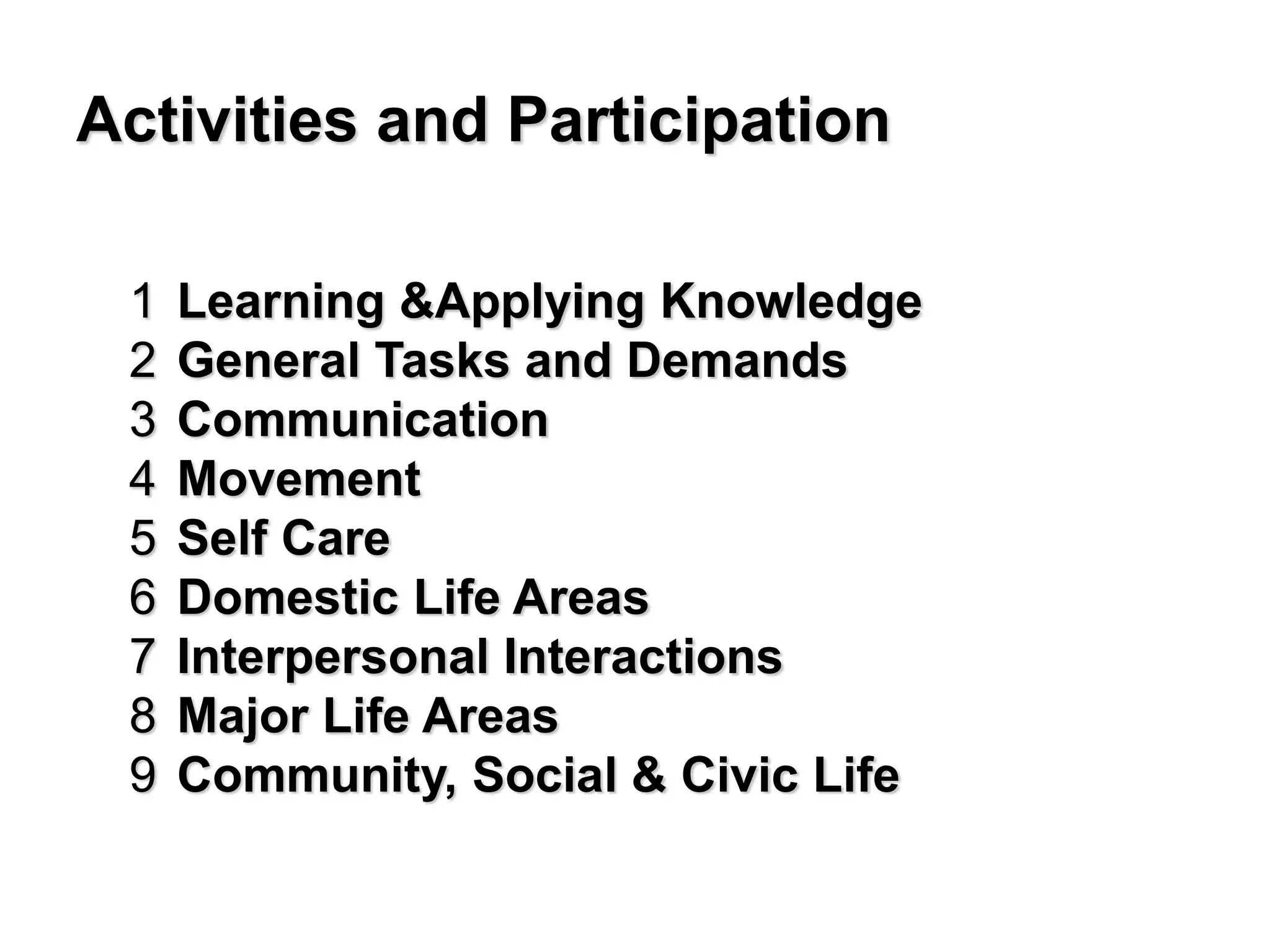


The document discusses the International Classification of Functioning (ICF) framework developed by the World Health Organization (WHO). It provides a standardized language for classifying and describing human functioning and disability. The ICF aims to establish a common language to improve communication about health and disability across countries, disciplines, services and time. It takes a holistic and interactive approach by considering body functions and structures, activities, participation and environmental factors. The ICF can be applied across various sectors like health, education, labor and policymaking.